ANVS - Alzheimer's Disease Drug Development: Another Lost Year
2023-12-05 03:58:10 ET
Summary
- Investing in most current Alzheimer's drug companies is not recommended because they are not likely to modify the disease.
- Compounds that inhibit oxidative stress may only slow down the progression of Alzheimer's disease over the short term.
- Anavex's blarcamesine, Cyclo Therapeutics Trappsol Cyclo, Green Valley's GV-971, aromatherapy, and panax ginseng not only inhibit the formation of oxidants but scavenge them and reverse part of their damage.
- Drug candidates and natural products such as these may arrest the progression of mild Alzheimer's disease for years and modify the progression of moderate Alzheimer's disease.
In this article, I will explain why I don't recommend investing in most current Alzheimer's drug companies. Some of these companies are working on other indications with other drugs (or in some cases the same drug) and a few such as Eli Lilly ( LLY ) have been tremendously successful at this to date. For many of these companies, though, the outcomes of their Alzheimer's disease trials are critical to their fates. Why they are not likely to be successful is of utmost importance for investors. More importantly, understanding the reasons why Alzheimer's trials keep failing is critical to prompting a new course of action against the disease.
Before discussing the reasons why the current approaches to Alzheimer's disease are likely to produce middling results, I will briefly summarize a few of the major developments of the last year.
In a year in which the Food and Drug Administration has approved a second anti-amyloid drug for Alzheimer's disease and is poised to approve a third, it may seem odd to describe it as another lost year. However, the FDA's approval of Leqembi was only a (fleeting) success for Biogen ( BIIB ) and Eisai ( ESALY ), for the FDA, for the proponents of the amyloid hypothesis of Alzheimer's disease, and for Alzheimer's advocacy groups such as the Alzheimer's Association. It was not a victory for those with Alzheimer's disease and their caregivers.
In some ways, the FDA's approval of Leqembi was a failure. The agency simply approved another drug for Alzheimer's disease that has minimal effectiveness. Its willingness to approve a drug based more on biomarker data (the removal of amyloid) rather than on any evidence of disease modification was misguided. By approving Leqembi, the FDA gave new fuel to efforts to treat Alzheimer's by reducing or eliminating amyloid rather than through other means. Unintentionally, though, it gave hope to every company whose drug candidate was likely safer than Leqembi and was at least as efficacious as Leqembi albeit for shorter periods of time.
The other apparently decisive news of the year came recently from BioVie. BioVie's struggle to achieve statistical significance for its drug candidate NE3107 was yet another setback in the effort to find an effective treatment for Alzheimer's disease. In sites removed from the study due to alleged misconduct, some patients on placebo also improved. While this is somewhat unusual, it is not unheard of in shorter-term trials. The impact of Alzheimer's medications or other treatments can result in short-term improvements in those on placebo. More importantly, a longer-term trial is needed to see whether a drug candidate produces separation from placebo or not (from 12 to 18 months for Alzheimer's disease and up to three years for mild cognitive impairment).
Moreover, the contention that patients improve the longer they are on the drug has so far been disproven by almost every drug developed for Alzheimer's disease. Aricept/donepezil was initially approved on short-term data. After one year the drug has almost no effect on those with mild Alzheimer's disease ( table 3 ) and has little effect on those with moderate Alzheimer's disease from the beginning ( study ). The anti-amyloid drugs are somewhat of an exception because it appears to take time to remove amyloid, but once the amyloid is removed the disease likely progresses at the same rate as before (for those in whom amyloid is contributing to the disease progression). In any case, the argument that a drug should be approved on short-term data (6 months to 12 months) because it performs similarly to Leqembi at 18 months is unlikely to move the FDA. While not entirely oblivious to the problems surrounding anti-amyloid antibodies, the agency will likely be looking for a future drug that is clearly superior to the existing standard of care in terms of efficacy.
Now, here are the reasons why the current approaches to Alzheimer's disease and the treatments based upon them are not likely to produce any resounding successes.
Anti-Amyloid Antibody Drugs
Again, one could argue that anti-amyloid drug companies have been successful. Biogen and Eisai have had two drugs approved for the treatment of mild Alzheimer's disease: Aduhelm and Leqembi. Eli Lilly is likely to have its drug candidate - donanemab - approved relatively soon as well. But in terms of the effective treatment of Alzheimer's disease none of these drugs do much.
Biogen, Eisai , and Eli Lilly have at various times acknowledged that their drugs are not effective for non-APOE4 carriers. For aducanumab/Aduhelm, the FDA statistician confirmed this ( report, p. 12/58 ). In its phase 3 clinical trial for lecanemab/Leqembi, Biogen and Eisai stopped comparing the declines in non-APOE4 carriers and APOE4 carriers against the placebo group for each and compared them against the combined placebo group. Here is a simple illustration of how this distorts the data: if non-APOE4 carriers on placebo decline by .5 points at eighteen months and APOE4 carriers on placebo decline by 1.5 points at eighteen months, the combined placebo decline is 1 point. If non-APOE4 carriers on the drug decline by .4 points at eighteen months and APOE4 carriers on the drug decline by 1.2 points at eighteen months, then against a combined placebo non-carriers "improved" by .6 points (1- .4=.6) whereas carriers got worse by .2 points (1 - 1.2=-.2). But when compared to their own placebo group, non-carriers declined by .1 points less (.5- .4=.1) than those on placebo whereas carriers declined by .3 points less (1.5- 1.2=.3). The FDA, in essence, has approved an expensive drug administered intravenously that has essentially no effect on non-carriers and which carries the risks of brain bleeds and brain swelling in carriers.
In APOE4 carriers amyloid levels are high enough to activate various receptors that contribute to oxidation and nitration in Alzheimer's disease. That does not appear to be the case for non-carriers. Amyloid is one of many factors that can activate receptors that initiate Alzheimer's disease, so its removal only has a slight effect and then only in APOE4 carriers (perhaps minimally clinically significant in some APOE4 carriers). In APOE4 carriers, the removal of larger amounts of amyloid in blood vessels can result in edema (swelling) and micro-hemorrhaging (brain bleeds) which can result in death.
Biogen with its current pipeline seems destined to remain in the low to mid 200s. Concerns about how much Leqembi will actually be prescribed and likely competition from Eli Lilly's donanemab will further eat into profits, putting a ceiling on the stock's value. On the other hand, Eli Lilly has escaped the Alzheimer's trap by developing a successful drug for type 2 diabetes and weight loss - Mounjaro. So far stomach paralysis has been the most serious side effect reported after taking the drug. At this point, it does not look like there is a countervailing force to bring the company's stock value down (except if more negative patient reports from the long-term use of Manjuaro begin to appear). It is possible, on the other hand, that the approval for donanemab may give the company a little further boost.
Anti-Amyloid non-Antibody Drug Candidates
A number of companies are working on drugs that prevent the development of amyloid oligomers and plaques in the first place. The furthest along of these is Alzheon's ALZ-801 (a prodrug of homotaurine), which prevents the aggregation of soluble amyloid into oligomers and plaques. Alzheon is developing the drug for APOE4 carriers, after discovering that it did not help non-carriers ( finding ). ALZ-801 does not cause brain swelling or brain bleeds because it does not remove amyloid. Preventing the aggregation of amyloid should be just as effective as removing it, so it is possible that ALZ-801 is just as effective as anti-amyloid drugs in APOE4 carriers but without side effects. The same may also be true of Annovis' ( ANVS ) buntanetap, which aims to prevent the formation of the amyloid precursor protein. To the extent that it also inhibits oxidative stress, buntanetap should also help non-APOE4 carriers to a certain extent.
Anti-Inflammatories
There are several drug candidates that fit into this category, but the one currently attracting the most attention is INmune Bio's ( INMB ) XPro1595. This proprietary compound inhibits the formation of a form of tumor necrosis factor that contributes to oxidative stress in Alzheimer's disease, but this is also true of many other cytokines and other inflammatory mediators. Inflammation has become one of the leading alternatives to the amyloid hypothesis of Alzheimer's disease, but both amyloid aggregation and inflammation are the results of oxidative stress and both are secondary triggers (in some cases) for the disease. Reducing neuroinflammation may for a period of time slow the progression of the disease, but it is unlikely to modify the disease.
Inhibiting the Pathways that Lead to Oxidative Stress
Many drugs fit into this category including the acetylcholinesterase inhibitors, some of which like Aricept are also s igma-1 receptor agonists , and Namenda/memantine. Sigma-1 agonists limit the production of oxidants early in Alzheimer's disease by inhibiting the release of intracellular calcium. They thus slow down the advance of mild Alzheimer's disease for about a year. In addition to Aricept, other potential treatments in this category include Anavex 2-73/blarcamesine ( AVXL ) and possibly Cassava Sciences' ( SAVA ) simufilam (the latter "conclusion" is based on simufilam's chemical structure and its nearly identical results to Aricept, and not on any direct findings). I will discuss what makes blarcamesine somewhat different from other sigma-1 receptor agonists later on.
Many of the early pathways leading to Alzheimer's disease and its early progression are downregulated as the disease progresses ( one example ). Compounds that intervene later in the disease process (from NMDA overactivation to peroxynitrite formation and caspase-3 activation) have a better chance of slowing the progression of moderate Alzheimer's disease for a while ( pathway graph, figure 3 ). This includes BioVie's NE3107 which by limiting the phosphorylation of ERK inhibits the production of peroxynitrite ( study ). Slowing the production of oxidants, however, only slows down the progression of Alzheimer's disease for a while.
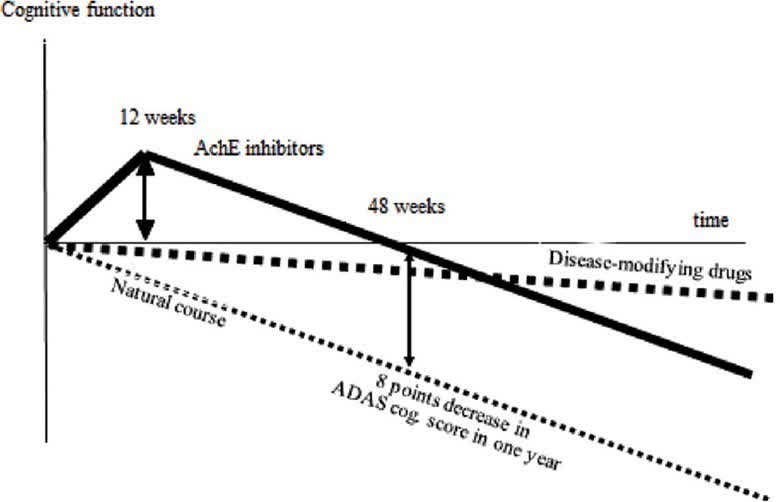
Disease Modifying Treatments for Alzheimer's Disease
Disease modifying or arresting treatments for Alzheimer's disease in addition to slowing down the production of oxidants also scavenge oxidants (such as hydrogen peroxide and peroxynitrite) and reverse part of the damage they do to the brain. Visually the difference between "symptomatic" and disease altering treatments can be seen in the chart below:
Disease Modifying (Alzheimer's and Dementia)
{kind=link}
Compounds that not only prevent the production of oxidants (often at multiple points such as inhibiting phospholipase C activity, reducing the size of lipid rafts by lowering cholesterol levels in the brain, and by inhibiting nuclear factor Kappa beta) but also scavenge them and reduce the damage they do the brain can potentially stop the progression of mild Alzheimer's disease for years. For moderate Alzheimer's disease, they may only modify the disease due to higher levels of oxidative stress at this point (see chart below for some validation of this supposition).
Chinese herbs (BMC Complementary Medicine and Therapies)
CT: Conventional therapy, mostly donepezil but in some cases also memantine.
H: A series of Chinese herbs (see article for list).
The primary nitro-oxidant in Alzheimer's disease is peroxynitrite. The likely key to treating the disease is contained in this quote:
The inflammatory mediator peroxynitrite, when generated in excess, may damage cells by oxidizing and nitrating cellular components. Defense against this reactive species may be at the level of prevention of the formation of peroxynitrite, at the level of interception, or at the level of repair of damage caused by peroxynitrite ( source of quote ).
The drug candidates and natural products that do all three have produced positive results for the treatment of Alzheimer's disease. By partially reversing oxidation and nitration, they have increased levels of neurotransmitters needed for the retrieval of short-term memory, sleep, balanced mood, social recognition, and alertness, improved neurotransmissions, and decreased neuronal cell death.
On a last general note before examining drug candidates and natural products that appear to arrest mild Alzheimer's disease, much has been made of using biomarkers to deduce the possible success of treatments for Alzheimer's disease. The exact relationship of these biomarkers to Alzheimer's disease is not known, however, nor how much levels would have to change to have an impact on the disease. Having said this, one of the most accurate biomarkers for Alzheimer's disease is declining levels of the brain's main antioxidant glutathione. Indeed, the decline in glutathione levels exactly matches the locations and progression of Alzheimer's disease:
The hippocampi - the brain centres for learning and memory - are one of the earliest regions to be sabotaged by Alzheimer's pathology. Our data revealed that GSH (glutathione) levels plummet in the hippocampi of patients with Alzheimer's as well as those with MCI [Mild Cognitive Impairment]. The frontal cortices - brain CEOs [Chief Executive Officers] responsible for a variety of executive functions - are chronologically affected later in Alzheimer's. GSH levels mimic this chronology with no changes in the cortices of MCI patients, but significant reduction in those of Alzheimer's patients. Interestingly, GSH remains unaffected in the cerebellum - a brain region unaffected by Alzheimer's till late stages. It appears GSH decline is not ubiquitous but rather a region specific phenomenon that appears to precisely map the progression of Alzheimer's in our brains ( source of quote ).
Glutathione does not readily enter cells and some of its precursor molecules cannot be transported into brain because of the oxidation of transport systems. External antioxidants cannot take the place of glutathione but they can reduce oxidative and nitrostative damage on their own and they can allow for some increase in glutathione levels.
It is now time to look at the results of drug candidates and natural products that inhibit the formation of peroxynitrite, scavenge them, and repair part of their damage.
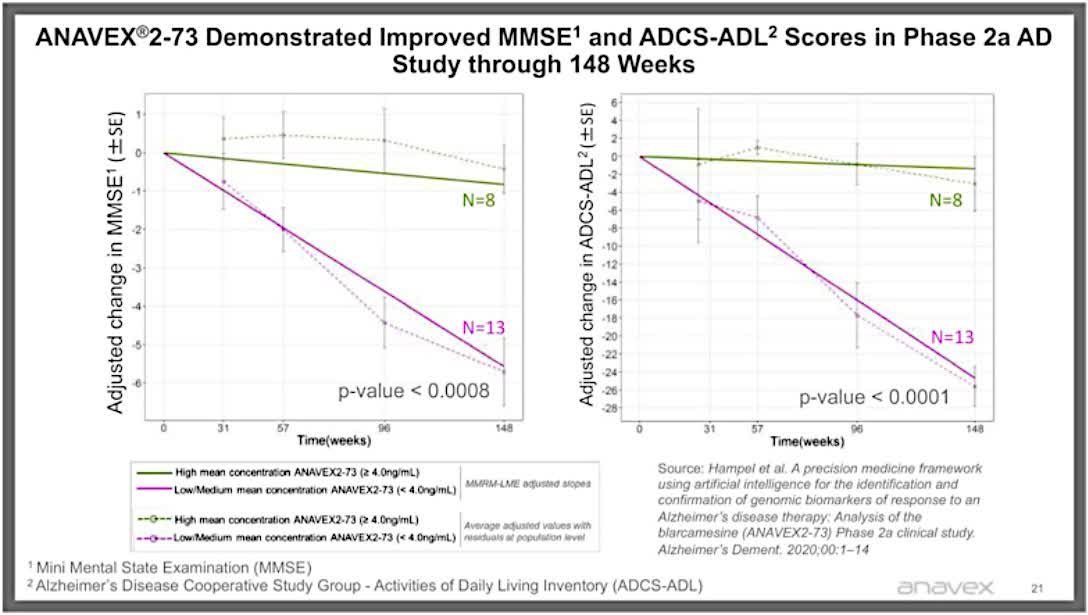
Anavex 2-73/Blarcamesine
Anavex 2-73 has produced cognitive improvements in some patients at 57, 70 , and 148 weeks. These patients share the following characteristics: high concentrations of the compound, mild cognitive impairment or mild Alzheimer's disease, functioning sigma-1 receptor, and no COMT (Catechol-o-methyltransferase) variations.
Anavex 2-73 at 148 weeks (Anavex)
{kind=link}
Anavex's compound is a tetrahydrofuran derivative which potentially through the donation of electrons and hydrogen atoms scavenges peroxynitrite and in doing so partially reverses the oxidation and nitration of receptors, transport systems, and enzymes needed for normal brain function. Unfortunately, it appears that one of the potential metabolites ( gamma-butyrolactone ) that results from scavenging oxidants can cause confusion and dizziness. The dropouts and down titrations caused by these side effects in the high-dose group may have prompted Anavex to combine the results with the lower-dose group in order to achieve statistical significance. The company hopes that night-time dosing may reduce dizziness (perhaps as long as one does not have to get up during the night). It is now pursuing approval of blarcamesine for Alzheimer's disease through the European Medicines Agency. This strategy perhaps indicates resistance from the U.S. Food and Drug Administration, which may want a longer and larger trial for the high-dose group to determine safety and efficacy. After making several exclusions due to side effects and non-responding groups, blarcamesine does appear to stabilize mild cognitive impairment and mild Alzheimer's disease in some patients for at least three years at high concentrations/doses.
GV-971
Green Valley's GV-971 has been granted conditional approval for the treatment of Alzheimer's disease in China. The drug is an oligosaccharide derived from brown algae. The early short-term results were promising, but longer-term data is needed:
GV-971 (Alzforum)
Green Valley has subsequently suspended a very large multi-continental trial, but smaller trials continue ( article ).
Cyclo Therapeutics Trappsol Cyclo
Trappsol Cyclo is a polysaccharide. Cyclo Therapeutics has begun a phase 2b trial based on one case of apparent improvement in an Alzheimer's patient at 18 months.
After 18 months, the patient showed neurological and cognitive stability: this is a positive outcome given that persons with Alzheimer's Disease dementia are generally expected to decline during an 18-month timeframe. Speech fluency also improved as documents by the treating physician's report of a decrease in latency to word-finding. In addition, mood and behavioral features of the disease improved, such as less agitation, as noted by the patient, the patient's family and the treating physician ( source of quote ).
Phase 2b clinical trial results will indicate whether this was the exception or the rule.
Aromatherapy
Various essential oils contain compounds (for example, eugenol, geraniol, thymol, carvacrol) that have antioxidant effects. Others contain linalool (such as lavender) which may reduce anxiety and agitation. The more stimulating essential oils (cognitive-enhancing oils such as rosemary and bay laurel) can potentially increase blood pressure and increase anxiety.
The following clinical trial results suggest the positive effects of aromatherapy on Alzheimer's disease:
All patients showed significant improvement in personal orientation related to cognitive function on both the GBSS-J [Gottfries - Bråne -Steen Scale - Japanese] and TDAS [Touch-Panel Type Dementia Assessment Scale] after therapy. In particular, patients with AD showed significant improvement in total TDAS scores ( clinical trial ).
This trial did not specify the improvement in personal orientation but from my own experience it may include less trouble bathing, fewer delusions, less anxiety, better sense of time and place, better sleep at night, and more alertness and awareness.
The results for the second clinical trial are as follows:
Aromatherapy improves sleep quality in patients with AD, alleviated psychobehavioural symptoms, and improves quality of life. This effect of aromatherapy is probably caused by regulating oxidative stress damage in the brain and inhibiting the express of inflammatory factors to delay deterioration of AD. In fact, the method of stimulating the olfactory nerve though scent exposure is easy to implement because of its low invasiveness and is suitable not only for patients with AD, but also for caregivers. Our research confirms the effectiveness of aromatherapy as a non-pharmacological intervention for the treatment of patients with AD, and its potential as a valuable option is worthy of widespread application at healthcare facilities, communities, and homes in the future ( clinical trial ).
Panax Ginseng
Of all the myriad botanical products studied for the potential treatment of Alzheimer's disease, the one currently with the greatest evidence behind it is panax ginseng. Panax ginseng/Korean red ginseng contains two important antioxidant compounds: saponins (specifically ginsenosides) and polysaccharides. The combination of these compounds may stabilize mild Alzheimer's disease for at least two years:
Panax ginseng for Alzheimer's disease (Journal of Ginseng Research)
The various compounds in panax ginseng appear to partially reverse all the major negative effects of Alzheimer's disease on the brain, including increasing neuronal regeneration in the hippocampus, increasing blood flow, improving neurotransmissions by returning to their normal form (via de-nitration), and reducing neuronal cell death ( study one , study two , study three ).
It is unclear if combining one or more of these treatments would have a greater effect than any one of them used separately.
Investment Advice and Additional Reflections
It is possible or even probable that all these potential drugs that inhibit the formation of oxidants will produce similar or slightly better results than the current standard of care and most or all will be safer than the anti-amyloid drugs approved by the FDA. The logical conclusion is that the FDA would then approve these drugs as well. But this is far from assured, so I cannot recommend investing in any company whose compounds only modestly and temporarily slow down the progression of Alzheimer's disease. And from the standpoint of those with Alzheimer's disease or their caregivers taking a drug that is no better or slightly better than the current standard of care holds little appeal. On the other hand one of the drug candidates - blarcamesine - that may help stabilize mild cognitive impairment and mild Alzheimer's disease for long periods of time is in a kind of limbo because Anavex has yet to release the results for the higher dose group. The company is also unlikely to ever run a much larger trial to prove that blarcamesine has long-lasting effects on some of those with mild cognitive impairment and mild Alzheimer's disease. The other promising Alzheimer's drug candidate -Cyclo Trappsol - has yet to be tested in a clinical trial. Cyclo Therapeutics currently has a small market cap that will not change until (or if) it can complete its phase 2b clinical trial. From an equally challenging perspective, two of the most promising natural product treatments for Alzheimer's disease - aromatherapy and panax ginseng - have very few believers/supporters in the scientific community in the United States. This makes it extremely difficult to find funding to run large clinical trials for either one of them. And thus an effective treatment for Alzheimer's disease seems as far away as ever.
For further details see:
Alzheimer's Disease Drug Development: Another Lost Year