BIVI - BioVie: 9 Reasons For Enthusiasm
Summary
- Over the past few months, BioVie has reported good data from a Phase 2 trial in Alzheimer’s and a Phase 2 placebo-controlled Parkinson’s disease trial.
- The Phase 3 trial in Alzheimer’s is ongoing.
- Focusing on some of the trial’s endpoints, I set out why I think the recent criticism is unfounded.
Introduction
BioVie ( BIVI ) has, over the past few months, generated an exceptional amount of data on both Alzheimer's and Parkinson's disease. A total of five press releases have been issued on the subject since the announcement of topline data from the investigator-initiated Phase 2 trial in Alzheimer's. The corporate presentation has been updated accordingly, and the three posters/presentations of the company at the CTAD conference contained quite some data as well. The dataset has become large fast, and is quite a lot to take in. Some data was communicated preliminarily at first, and then final later. One should therefore pay close attention before making any judgments on the company.
Recent coverage on BioVie by Seeking Alpha author C.C. Abbott provided some points of criticism on the company's results and reporting.
The trading day after publication, the stock fell by 25%, and the day after 30%. That gives rise to an assessment as to whether any points of criticism have merit.
The comments and/or criticism in the earlier coverage come down to nine points, which I will set out below. I believe none of these are correct. I have therefore taken the liberty to correct them. In my corrections, I see nine points of enthusiasm. I have numbered them accordingly.
The stock has dropped massively since the publication of the afore-mentioned article, and I am seeing this as a buying opportunity. For that reason, I give a strong buy rating to BioVie.
BioVie's Phase 2 data in Parkinson's disease
BioVie has reported topline data from its Phase 2 placebo-controlled study in Parkinson's disease on December 5, 2022. It mentioned five points, in essence.
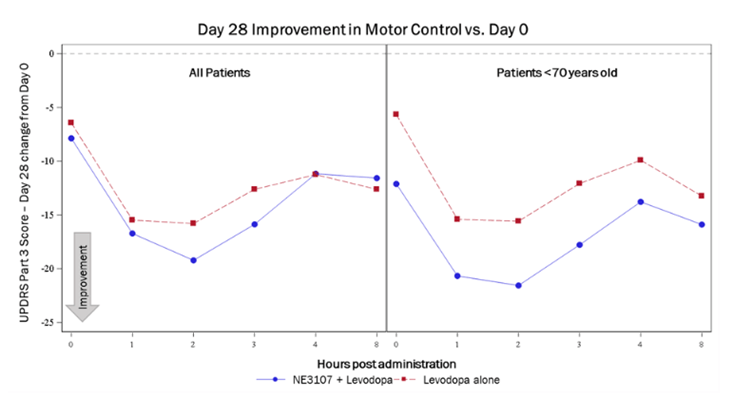
- NE3107-treated patients experienced greater motor control in Parkinson's trial.
- Patients treated with the combination of NE3107 and levodopa saw improvements in their UPDRS Part 3 (motor) score that is 3+ points superior to patients treated with levodopa alone, which is considered to be clinically meaningful by Parkinson's experts.
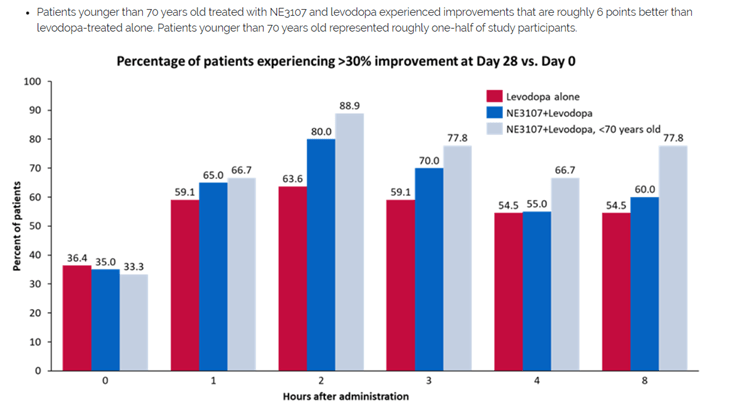
- Patients under 70 years of age treated with NE3107/levodopa experienced roughly 6 points superiority compared to those treated with levodopa alone, suggesting that younger patients with less advanced disease progression may experience greater impact from treatment with NE3107.
- 88.9% of patients <70 years old treated with NE3107 and levodopa experienced greater than 30% part 3 score improvements from baseline at the 2-hour mark compared to 63.6% of patients treated with levodopa alone.
- The study met both of its objectives.
The press release also mentioned, and I believe this is very important:
Full details from this trial will be presented at the upcoming AD/PD™ 2023 International Conference on Alzheimer's and Parkinson's Diseases to be held March 28-April 1, 2023 in Gothenburg, Sweden.
Importantly, also, at this time no per-patient data or p-values have been communicated.
To me, those results are in line with what had been hoped for. BioVie had seen a clear efficacy signal of levodopa and its drug candidate NE3107 combined in preclinical models. There were two underlying reasons for that. The primary reason is that NE3107’s reduction of inflammation takes away the primary factor underlying disease progression. Like Alzheimer’s, Parkinson’s disease is very much driven by immune-dysfunction. Lowering the inflammation should lead to a normalization of the immune system, and henceforth could halt or reverse the disease. Furthermore, as the levodopa-induced dyskinesia is related to inflammation, NE3107’s reduction of inflammation should be beneficial.
The data is strong, and like in Alzheimer’s, presents more strongly in a supposedly less-evolved or in any case less-aged subgroup (cfr. the aging claim), namely patients under 70 years old. The normal progression of Parkinson’s patients in UPDRS-Part III is a decline. That decline over a year’s time is in between 1.4 and 8.9 points (mean: 5,15). BioVie’s results show improvement at 28 days, with results on NE3107 outperforming standard of care levodopa by 3+ points in the entire group, and 6 points in the group of patients less than 70 years old. That is a definite and strong treatment effect, which I assume will continue the longer treatment takes.
The comments / criticism here as mentioned in the previous coverage are as follows:
- The 11 pre-specified endpoint results are not disclosed, hence it is unknown whether they support or contradict BIVI's claims that the trial has met its two design objectives.
- The data communicated by BioVie on motor control, UPDRS part 3, is not statistically-significant. That means a conclusion cannot be drawn from that data. That point is repeated three times.
My reply to these comments/criticism is as follows:
1. The data that has been released is supportive of enhanced motor control.
BioVie's press release included charts to show that enhanced motor control.
Company Presentation Company Presentation
{kind=link}
{kind=link}
BioVie’s press release also mentioned expressly that full details of this trial will be presented at the AD/PD conference in Gothenburg, Sweden. That data should therefore be awaited. At this time, though the company seems confident in them, nobody knows whether these values will be positive or negative. It is still possible that the company has tried to present available data in a good way, but making it appear as if the company has neglected to communicate this data even though the company mentioned that full data would be presented at a later time is incorrect in my opinion. A preliminary conclusion can be drawn from data that has been communicated by the company.
2. The full dataset is being prepared - considering that BioVie has failed to communicate it or that it would not be statistically significant is incorrect.
BioVie has not yet communicated any data per patient or p-values yet on its Parkinson's trial. Making (potential) investors believe that BioVie has communicated a full dataset, or a dataset with p-values, by concluding that the data that has been communicated is not statistically significant is incorrect.
BioVie's data in a Phase 2 trial for Alzheimer's disease
BioVie has reported quite impressive data coming out of its 3-month open label study in Alzheimer’s patients. A total of 23 patients had been treated, of which 18 patients had a Mini-Mental State Examination score of >20, and 5 a score of <20. Different measurements were taken. Several cognition scales have been used to assess patient’s disease progression or treatment effect, including several blood and neuroimaging biomarkers. Results – improvements - were strongest on Adas-Cog 12, a scale similar to Adas-Cog 11 which has been used by Cassava Sciences to report data. Alzheimer’s patients normally decline by 6-12 points on Adas-Cog per year, so about 1.5 to 3 points per 3 months.
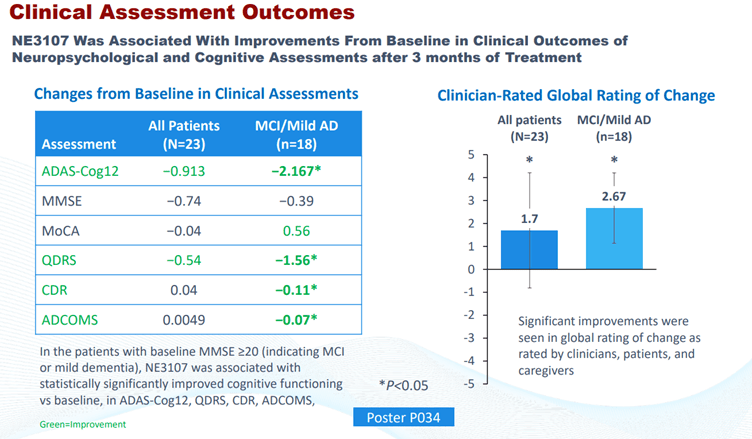
In all patients, treatment with NE3107 showed an improvement of 2.2 point on ADAS-Cog12 (p=0.0173), equating to 21.1% (p=0.0079) change compared to baseline.
Among only responders, the improvement was 3.7 points (p=0.0003) equating to 36.2% (p<0.0001) compared to baseline. The understanding of a supposed decline of 1.5 to 3 points per 3 months makes a 3.7 improvement over the same period, and a 2.2 point improvement in the entire patient group, very meaningful.
On other scales, improvements were also seen, including on the Severe Impairment Battery Scale or SIB, and for me the consistency here is of essence. For reference, Eisai used the SIB-SoB in its study of Lecanemab, where results were only visible after six months. NE3107 treatment showed an improvement of 0.11 (p=0.0416) on the Clinical Dementia Rating scale (CDR), equating to 19.4% (p=0.0416) change from baseline. Most interestingly here, as this is part of the mechanism of action for NE3107, improvements in inflammation correlated with those in cognition, with a p-value of p=0.0259. Other good results presented were on CSF phospho-tau, and the ratio of p-tau to A? 42 . Of 22 patients with abnormal baseline brain scans, 18 improved in one or more regions. Finally, NE3107 treatment in Alzheimer’s disease appeared to reverse DNA methylation – biological aging, so to speak - by 3.3 years over the course of 3 months. Insofar as I know, nothing even coming close to that has been reported before.
The comments / criticism to BioVie's reporting here is as follows.
- BioVie has focused on reporting data on cognition, though measurements here were actually secondary endpoints.
- BioVie has reported four cognition measurements, namely ADAS-Cog, CDR, ADCOMS and Global Rating of Change. Two of these are per protocol. BIVI did not disclose Montreal Cognitive Assessment (MoCA) and MMSE results.
- BioVie has reported on several biomarkers that are not pre-specified endpoints, namely TNF?, CSF phospho-tau level, the ratio of p-tau to A?42, and the Horvath DNA methylation SkinBlood clock. The latter is not an endpoint in any other AD trials I'm aware of. Its validity and usefulness as supportive data in the NE3107 data package are questionable.
- Among the five pre-specified biomarker endpoints, only the first, i.e., advanced functional MRI results, was mentioned.
- What happened to the 23rd patient?
- Non-placebo-controlled data cannot be used to report statistically-significant improvements in cognition. There is no reliable way to separate the treatment and placebo effects. The data on cognition could lead to an early 'probable' signal at best.
My comments to these comments and/or points of criticism are as follows:
3. Cognition is key
Alzheimer's disease is essentially a disease that comes with loss of cognition. Cognition is key, and if a trial can show an improvement of cognition in a quite considerable amount of patients, then it should be the company's prerogative to communicate such, all the while informing investors that the full dataset would be presented at CTAD 2022. At this conference, the data has been separated in three packages: clinical outcomes – cognition, biomarkers and neuroimaging data. These three packages have been presented separately. There is nothing wrong with that.
4. BioVie has disclosed all of its predefined cognition measurements
The company has included other measurements as well. There is nothing incorrect about that. It is, on the contrary, incorrect to consider that BioVie has not disclosed Montreal Cognitive Assessment (MoCA) or MMSE results, even though they had been prespecified.
{kind=link}
On the last slide, note that green is improvement. What is not green, does not mean that patients' cognition is going down like normal Alzheimer's patients. Besides, one again sees the consistent effect in MCI/mild AD patients. The MoCa score in all patients shows stabilization, where it shows improvement in MCI/mild AD patients. As to the comment that MoCA and MMSE results are mixed and not as strong as other data, this is an interesting one too, I believe. In analyzing a company, I believe there should not be a full disregard of all the good data, in an effort only to find points of criticism. The MoCA and MMSE data are still much stronger than any data Biogen ( BIIB ) has ever reported with Aduhelm, or Eisai with Lecanemab.
The fact that consistent changes are shown across multiple cognition scores has correctly led to considerable enthusiasm. That is unseen. The correlation between all cognition scores is meaningful as well, as it could be indicative of a future outcome. The trial may not be placebo-controlled, but the fact that cognition does not decline like it does in normal Alzheimer's patients on most cognition rating scales, is meaningful.
Company Presentation
Imagine BioVie would have shown these results ( link to PR ):
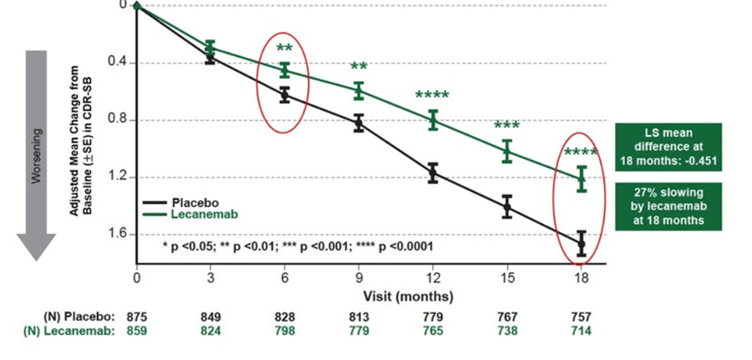{kind=link}
These results have led to market cap increases in the billions of dollars. All-in-all very moderate, compared to the above, I would say. Well, the above results come from a Phase 3 trial of Eisai with Lecanemab. That got the stock market excited. I'm happy for Eisai, but NE3107 appears to do much better. However, the upcoming phase 3 will allow us to follow vet this point.
5. Biomarker endpoints have been communicated
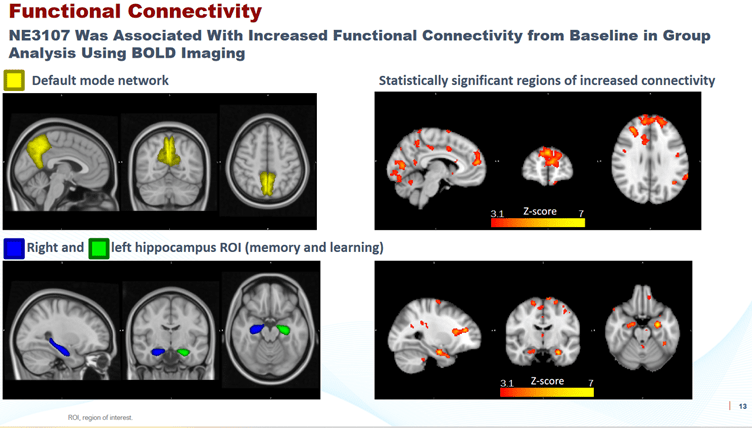
Another point of criticism is that among the five pre-specified biomarker endpoints, only the first, i.e., advanced functional MRI results, was mentioned. Again, this comment which was repeated twice is very much incorrect. These endpoints had been communicated before, and have meanwhile been included in the corporate presentation or have been presented at CTAD.
Results on endpoint 4 - fMRI Bold - had been published before, has been included in corporate presentation, and has been presented at CTAD as well.
{kind=link}
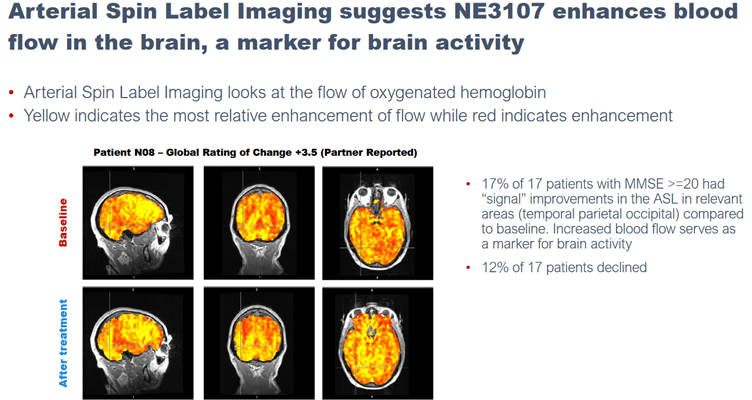
Results on arterial spin label imaging had been published before, and had been incorporated in the corporate presentation.
{kind=link}
On endpoint II, the slideshow presented at CTAD mentioned that the data analysis was still ongoing, so these results are still awaited.
{kind=link}
6. Additional information, additional confirmation
As to the allegation that the company has communicated biomarker data that weren't pre-specified, I don't really see the issue here. The company and certainly the investigator should be free to do any assessments. TNF? is highly relevant because it underscores the basis of NE3107. CSF phospho-tau level and the ratio of p-tau to A?42 are standard measures in Alzheimer's disease, and very much relevant. The results here should be applauded instead of criticized.
7. Reversing aging in an age-related disease
Assessing DNA methylation by the use of an innovative method such as the SkinBlood clock is state-of-the-art. The related press release was also separate from the others. This information actually has the potential to be significant, not so much as an age claim, but as a clear and perhaps first proof in diseases of aging that NE3107 has a strong effect. Dr. Horvath's aging clocks are renowned.
If a drug candidate can in 3 months' time turn back the aging clock by 3.3 years, obviously something is going on in the patients' bodies. Researchers have observed inflammation being associated with hypermethylation. NE3107 reduces inflammation. Simply dismissing that information as it's too novel, or a framework in current Alzheimer's thinking is not available yet, is not appropriate in my eyes.
BioVie's recent letter to shareholders sets out the framework to understand this information, with sixteen references to publications:
Data shows that treatment with NE3107 for three months showed a reduction of 3.3 years (p=0.0021) using the Horvath DNA methylation SkinBlood clock. Furthermore, 19 out of the 22 patients experienced this reduction in the SkinBlood clock score. […]
There’s an increasing body of evidence that signs of aging are epigenetic in nature. Perhaps the most studied area of epigenetics involves DNA methylation, which is the process of how methyl groups are added or removed from DNA and thus regulate the expression of various genes in our bodies. 3 Many studies have shown that genes become over- or under-methylated as we age, thereby suggesting that the modulation of DNA methylation could enable the up- or down-regulation of specific genes and thus modulate the aging process.
Dr. Steven Horvath, Professor of Human Genetics at the UCLA David Geffen School of Medicine and Professor of Human Genetics & Biostatistics at the UCLA Field School of Public Health, is a leading authority on the study of DNA methylation, and his research publications have been cited nearly 90,000 times in peer-reviewed articles. Professor Horvath studied a large number of datasets comprised of most tissue and cell types to create the first epigenetic clock (or “biological clock” to measure “biological age”) to measure the cumulative methylation of selected sites in the genome and how this could differ from a person’s “chronological age.”
This finding that NE3107 may affect DNA methylation would be consistent with the understanding of its mechanism of action. NE3107 has been shown to modulate the expression of TNFa, which is considered to be the master regulator of inflammation. Inflammation has been shown to be associated with hypermethylation of DNA, which in turn has been shown to impact a wide range of diseases, including various forms of cancers, age-related cognitive impairment and dementia, Parkinson’s disease, cardiovascular disease, COPD and respiratory disease, chronic kidney disease, inflammatory bowel disease, sepsis, and many others.
I believe this encouraging finding that NE3107 may affect the biological markers associated with aging helps explain the results we have seen from our trials in Alzheimer’s and Parkinson’s, both diseases are associated with aging. NE3107 has shown the ability to modulate inflammation and insulin resistance by reducing TNFa, which leads to improvements in a series of downstream factors such as metabolic dyshomeostasis, apoptosis, oxidative stress, among others. NE3107’s impact on DNA methylation helps explain the magnitude and rapid pace of impact we see in the AD and PD trials.
8. Correct communication
Another question or point of criticism was what happened to the 23rd patient.
If that comment refers is to this press release mentioning "18 of 22 patients with abnormal baseline scans showed improvement in one or more brain regions as seen from advanced functional MRI studies", then it can be that one patient may not have had abnormal baseline scans.
In some cases not all patients were measured, but the data that had been presented mentioned that in such case. The poster presented at CTAD also mentioned that the study was not formally powered, and that 23 patients were enrolled assuming, from prior experience, that approximately 20 patients would complete the study.
9. The Phase 2 data give an indication of things to come
If one considers that the cognition data that have been communicated could point to an early 'probable' signal, that's exactly what BioVie has always communicated on these results, both in its letter to shareholders of October 4, 2022, and at CTAD in the neuroimaging presentation:
Although additional randomized, controlled studies are required to draw clinically meaningful conclusions, when the data is taken in its totality, it suggests that certain changes may be taking place in the brain that are consistent with NE3107’s mechanism of action and are unlikely to be accounted for by placebo effects.
All of this gives us encouraging signs of what we will hopefully see from our Phase 3 in AD that is expected to read out mid-2023.
{kind=link}
BioVie has always mentioned that the data coming out of the non-placebo-controlled Phase 2 data should be assessed with caution, exactly because it is not placebo-controlled. That does not mean that measurements are false in any way, or that an analysis of this data is not possible, to the contrary. BioVie has openly stated at several occasions that it is looking forward to its placebo-controlled data coming from a Phase 3 trial.
The fact that the same drug is able to additionally show improved motor control on short notice in combination with levodopa adds to the conviction that this drug has something to offer to patients with Alzheimer's and Parkinson's.
BioVie currently has a $200 million market cap
I’m currently basing my estimates on a 6.1 million patient population for Alzheimer’s disease, and a 1 million patient population for Parkinson’s disease. I am not including the numbers for BIV201, although this is actually a very de-risked and far-progressed asset with about $450 million in sales potential.
At a yearly cost for NE3107 of $25,000 in only 10,000 patients (1/700 th of the market), turnover could be $250 million. There are 7 million people diagnosed with Alzheimer’s and Parkinson’s in the US alone. Assuming a market share of 10%, which is moderate as NE3107’s potential is higher than Eisai’s Lecanemab in my eyes, potential peak sales could be $17.5 billion. A current biopharma revenue multiple of 8.9 could in such a case lead to a $155.75 billion valuation.
Given BioVie’s current market cap of less than $200 million, it is my view that, in spite of the excellent results and very far pipeline progression including a Phase 3 trial underway in the biggest indication, the market is currently giving BioVie a less than 1% chance of actually reaching a 10% market share one day. Hence, I believe there is tremendous upside to this stock.
Conclusion
Over the past two trading days, BioVie has lost pretty much half of its market cap.
Criticism has been uttered as to the reporting by the company over the past few days. I believe that criticism is not justified.
Admittedly, the data flow that has been generated by the company has been massive. Some of the data was so novel that an appropriate framework for it was harder to find than usually. The company has however provided that framework, and hence that should be taken into consideration. A claim that a drug may seem to reverse aging in patients with a disease related to aging dysfunction is not random, but may touch the essence of the matter.
The company has correctly communicated that its results coming out of a Phase 2 trial are preliminary in that they are not placebo-controlled. These results are however strong and consistent, and may therefore be indicative of very good things to come, in my opinion. Communicating results on cognition scales, if they are so good, does not appear as incorrect, all the more so if they are accompanied by biomarker and neuroimaging data communicated by the company in press releases, in its corporate presentation and at the recent CTAD conference. Taken together, I believe the recent points of criticism are unjustified. I do not see a reason for investors to hold their enthusiasm.
BioVie is sitting on a 200 million market cap, with potential peak sales of 17.5 billion in the US alone if a 10% market share could be held. With these results, I believe there is much upside to the stock at this time.
For further details see:
BioVie: 9 Reasons For Enthusiasm