BIVI - BioVie Pharma; Bullish Long-Term But Bearish On Upcoming Phase 3 Readout
2023-08-18 19:19:57 ET
Summary
- BIVI is undervalued if successful in any of its 3 programs [Alzheimer's disease(AD), Parkinson's disease, resistant ascites], but short-term the stock price will depend on upcoming AD phase 3 results.
- BIVI will soon need to raise cash to support planned phase 3 trials for above indications.
- AD phase 2 results were promising, but study was too small and too short, and patients had much milder baseline cognitive impairement compared to patients enrolled in phase 3 study.
- Based on the above I expect that the phase 3 study will likely fail to meet its primary endpoint. Pending topline results, I am staying on the sidelines.
Overview of the thesis
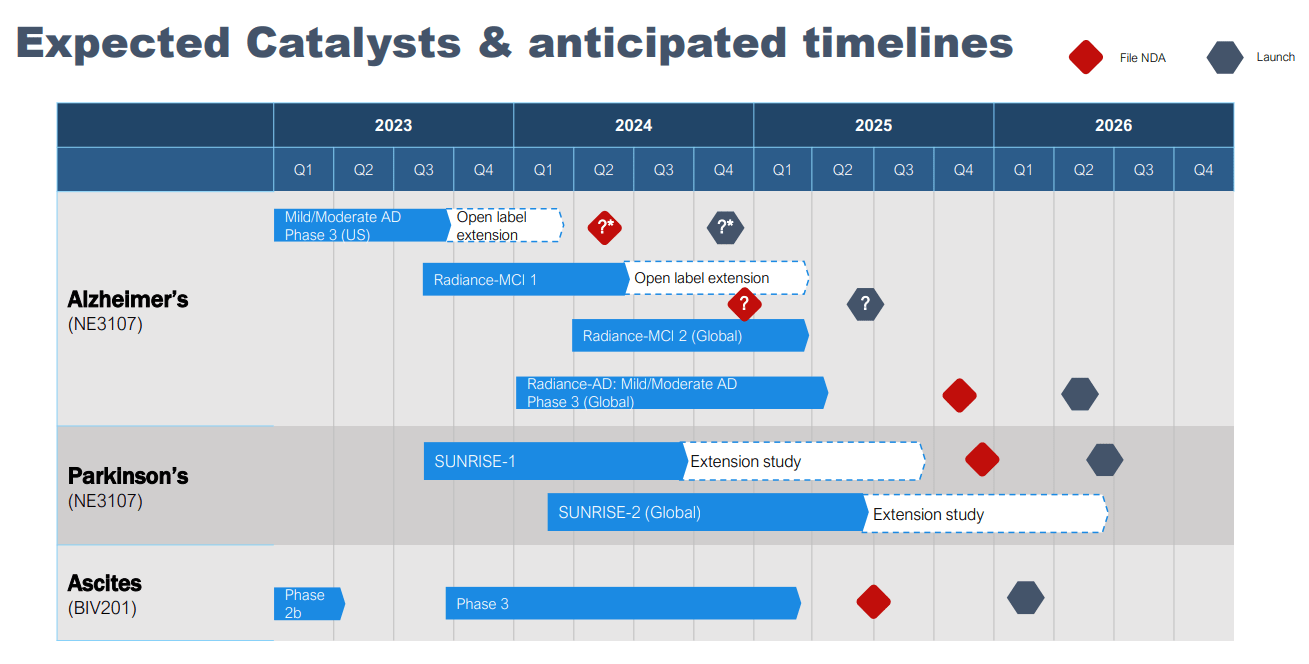
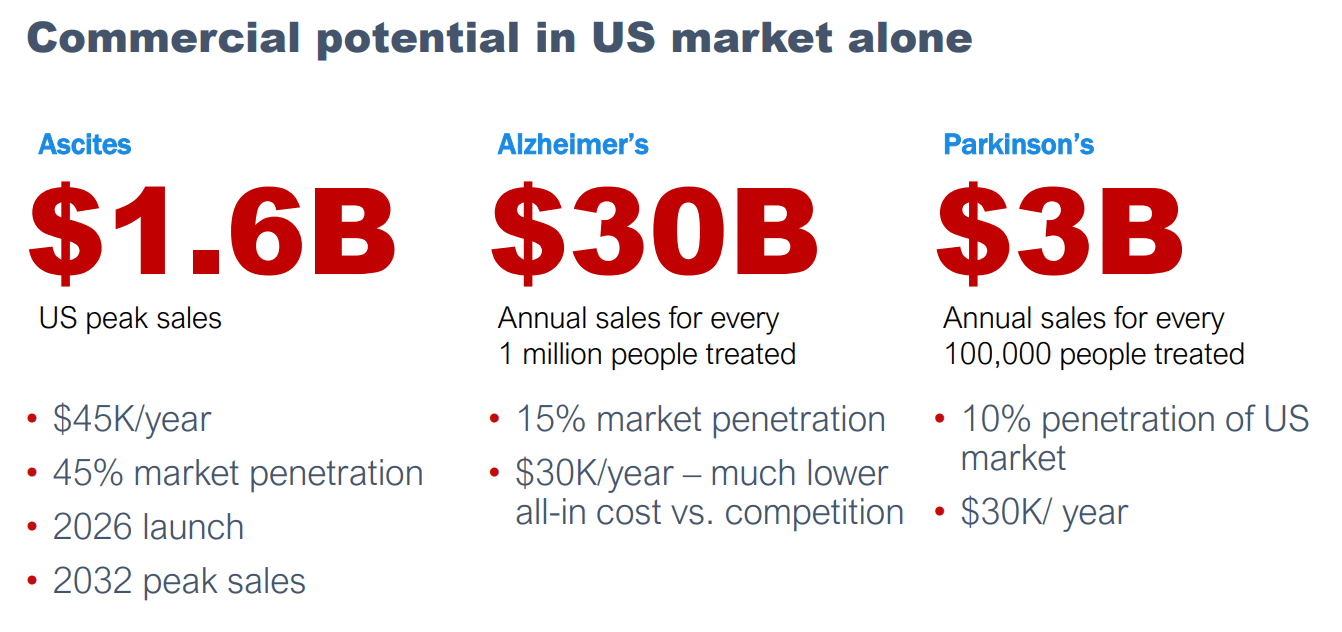
BioVie Pharma ( BIVI ) is developing NE3107 for Alzheimer's Disease (AD) and Parkinson's Disease (PD) and BIV201 for ascites (see pipeline in image below). All indications are phase-3-ready following promising results in phase 2 studies. BIVI estimates total peak sales potential of $34.6B for these 3 indications (see image below), by far the largest contributor being the AD indication (estimated peak sales $30B). Notably, BIVI has already completed a phase 3 study on AD with topline results expected in October/November this year. Considering BIVI's cash situation and cash needs (to support 6 planned phase 3 trials), failure to meet primary endpoint in AD phase 3 trial would be a major setback for BIVI and current shareholders.
Therefore, I chose to focus this article on BIVI's AD pipeline, and specifically on predicting the outcome of the phase 3 study, which I am afraid will fail to meet its primary endpoint. BIVI has elected to go directly to a phase 3 AD study despite the very small size (n=23) of the phase 2 study, which is a risky choice in my opinion. Furthermore, the phase 3 population (mild-to-moderate AD) is very different from phase 2 population (MCI/mild AD). Much worse baseline cognitive impairement (i.e. more difficult to treat) in phase 3 study, combined with relatively small study size and relatively short study duration all point that the phase 3 trial may be underpowered.
Considering the above I recommend BIVI as a "Hold" and I plan to re-assess following phase 3 topline results.
Biovie's company presentation Biovie's company presentation
{kind=link}
{kind=link}
Brief overview of PD, ascites and epigenetics pipeline
For a more detailed overview of the PD, ascites and epigenetics pipeline I refer readers to prior SA articles by E. Roudasev and Jacob Braun .
Briefly;
- BIVI has completed a double-blind, placebo-controlled phase 2 study in PD, including n=45 participants. Patients were treated for 28 days with carbidopa/levodopa and NE3107 or carbidopa/levodopa and placebo. The study showed enhanced motor control in NE3107 patients. The study also found that NE3107-treated patients experienced fewer motor symptoms before morning drug administration. This is important because many PD patients experience worsening of their symptoms ("off state") before their next levodopa dose. NE3107 benefits were more pronounced in younger (<70 years-old) patient. BIVI is planning two phase 3 trials in PD aiming for NDA filling in the end of 2025, and commercial launch in mid 2026.
- BIV201 (ascites indication) is terlipressin administered as continuous infusion in the outpatient setting using a portable infusion pump. BIV201 has Orphan and Fast track designations for treatment of ascites. BIVI has elected to terminate the ongoing phase 2b trial prematurely based on promising results from the first 15 (of 30 planned) patients. BIV201 combined with standard of care resulted in a 34% reduction in ascites fluid volume during the 28 days after treatment initiation compared to the 28 days prior to treatment (p=0.0046). Among patients who completed 2 X 28-day cycles with BIV201 results were even more impressive (53% reduction, p=0.001)(five patients discontinued treatment during or at end of Cycle 1). For comparison, in the standard of care group ascites volume increased by 3.1%. The treatment was safe, well-tolerated, without unexpected serious adverse events. BIVI is planning a phase 3 trial, aiming for topline results in Q1 2025, NDA filling in mid-2025 and launch in early 2026.
- Epigenetics: NE3107 has been shown to reduce epigenetic changes (DNA methylation) caused by inflammation. Notably , NE3107 led to >50% reduction in DNA methylation which was equivalent to -3.3 years on the Horvath DNA methylation Skin Blood Clock (suggesting, in other words, younger biological age compared to baseline). Potential for partnership has been suggested based on these findings, however BIVI is still exploring how to proceed and what to do with these findings.
BIVI's aggressive clinical development program
As recognized even by BIVI management their clinical development program is quite aggressive;
- As will be discussed below the ongoing phase 3 trial was desinged and initiated without any prior clinical efficacy data in AD patients. In the meantime BIVI has recently announced plans for three more phase 3 trials in AD (2 trials in MCI and 1 trial in mild-to-moderate AD) following a single small (n=23) phase 2 study.
- In PD, BIVI has completed a small (n=45) phase 2 study before proceeding to phase 3 studies.
- With regards to ascites program, BIVI has prematurely terminated the phase 2b trial at just n=15 (vs planned 30) patients based on very positive interim results and is proceeding directly to a phase 3 trial.
The benefit of this risky approach is the potential to reach approval and commercialization much faster and at a lower cost than would be possible by doing more phase 2 studies before the phase 3 studies. On the other hand the purpose of phase 2 studies is to de-risk costlier, later stage programs. BIVI will need to raise a lot of cash to support the six planned phase 3 trials, with limited de-risking from phase 2 data.
To fund these programs BIVI is considering all options , including potential partnerships. According to BIVI initial conversations have been held with some companies (some interested in global rights, others in specific geographic regions), but most companies are awaiting phase 3 data readout.
Design, rationale, and supportive evidence for ongoing phase 3 AD study ( NCT04669028 )
BIVI has published a paper explaining the desing and rationale of the ongoing phase 3 study. The following are notable from this publication:
(1) It is surpising that design of the phase 3 study was based solely on pathophysiological rationale, NE3107's mechanism of action and safety and pharmacokinetic clinical data.
(2) At the time the phase 3 was designed, supportive (pharmacokinetic and safety) clinical data came from 3 phase I studies (one in healthy subjects, one in obese subjects with impaired glucose tolerance, and one in obese-insulin resistant subjects), 2 phase I/II studies (one in ulcerative colitis patients, and another in rheumatoid arthritis patients), and 1 phase II study (in type II diabetes patients). In other words there were no clinical efficacy data in AD patients available when the phase 3 study was designed! Of note BIVI acquired the biopharmaceutical assets of NeurMedix (including NE3107) in June 2021 and initiated the phase 3 study in August 2021. In other words, with the acquisition of NE3107, BIVI also "inherited" the phase 3 study.
(3) Study's population is mild-to-moderate AD patients, but there is no rationale at all offered for this choice. The more advanced AD patients are the more difficult to treat. Therefore, the choice to include moderate patients, without any prior clinical efficacy data, is surprising to me. Furthermore, although randomization is stratified by MMSE, a subgroup analysis for mild patients does not appear to have been pre-specified in the protocol.
(4) The planned study size ("approximately 316") was based on an assumed "2.5 point difference between NE3107 and placebo based upon the ADAS Cog12". However, there is absolutely no supportive evidence explaining the rationale of this assumption, let alone considering the fact that at that time there were no clinical efficacy data in AD patients!
(5) Co-primary endpoints were initially ADAS-Cog12 and ADCS-CGIC change from baseline to week 30 (of which initial first 4 weeks are for titrating NE3107 upwards to the target dose). I have 2 observations about this. Firstly, the rationale for just 30 weeks duration is not explained. Notably other AD phase 3 trials have used much longer durations: simufilam 12 months, aducanumab / donanemab / lecanemab 18 months. Secondly, the co-primary endpoint has been changed to CDR-SB as a single primary endpoint. To my knowledge, BIVI has not officially announced the rationale for this change.
Brief overview of phase 2 results and comparison with the phase 3 trial population
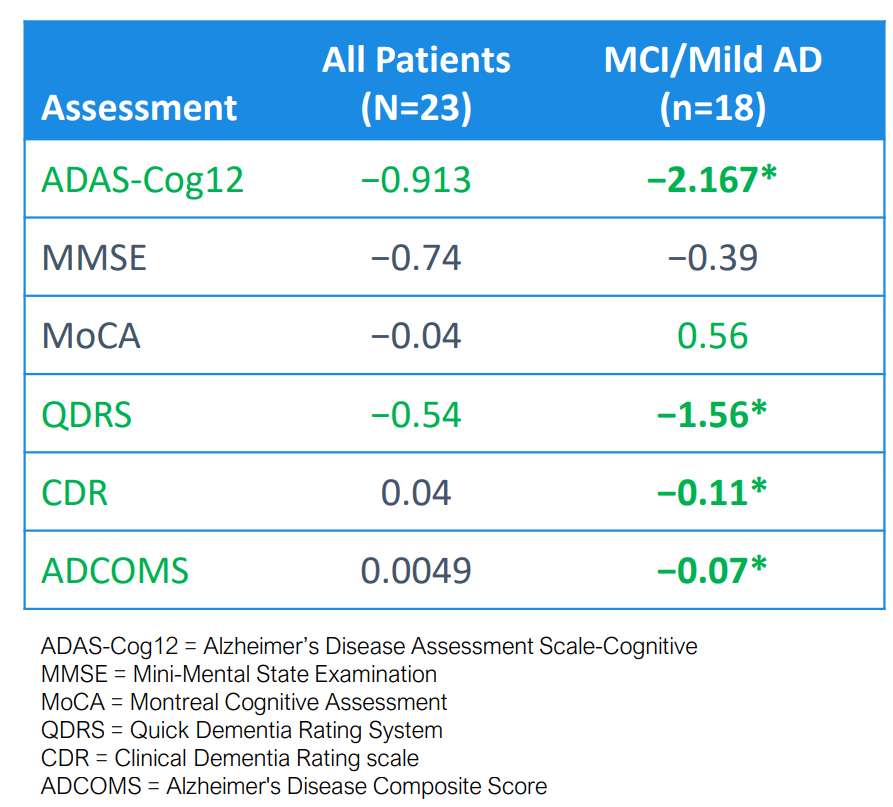
The phase 2 study was an investigator-sponsored open-label study that has enrolled n=23 patients, the majority (n=18) of which had mild cognitive impairment (MCI) or mild AD. All patients recieved treatment with NE3107 and outcomes were assessed at 3 months of treatment. Results in various cognitive assessment scales are summarized in Table below. Notably, CDR-SB (the current primary outcome of the phase 3) has not been reported in the phase 2 study. So, I will focus here on ADAS-Cog12, one of the original co-primary endpoints in the phase 3 trial. The study showed a decrease (improvement) of -0.913 considering all patients and -2.167 considering only the mildest patients, which is impressive for such a short duration of treatment.
{kind=link}
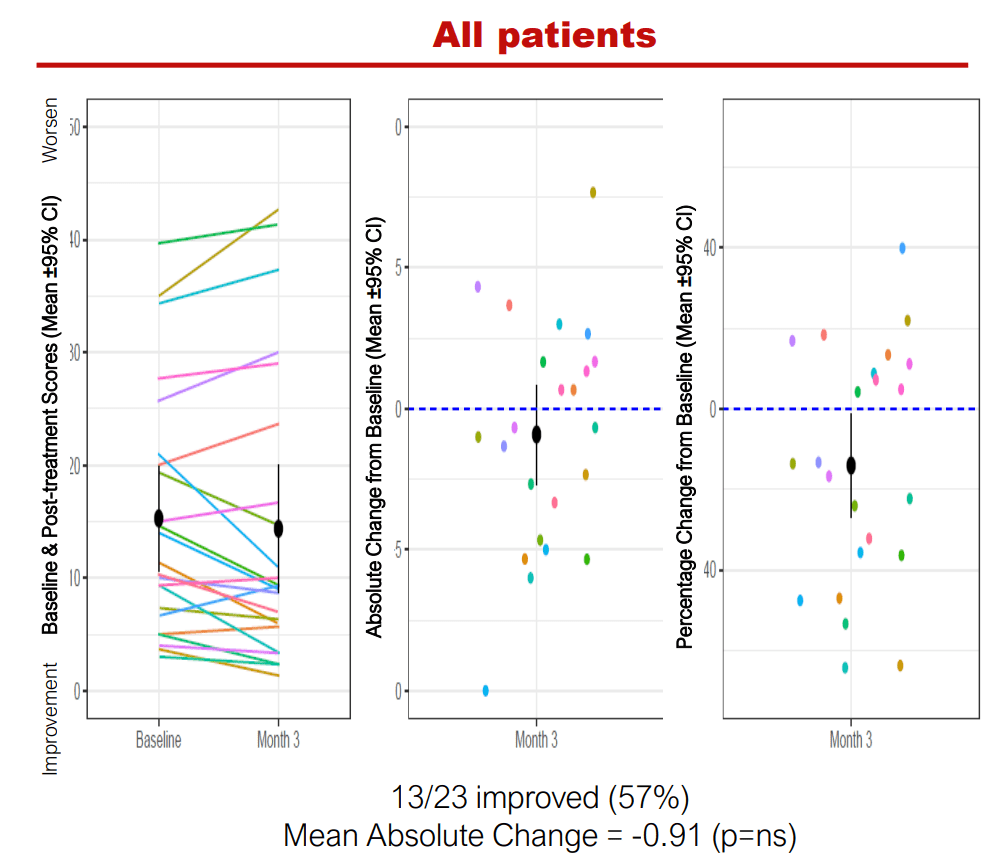
On closer look of the data (figure below) enrolled patients had a mean baseline ADAS-Cog12 score of about 15 (vs a mean baseline ADAS-Cog12 of 28 in the phase 3 study). InMCI/mild patients mean baseline ADAS-Cog12 score was even lower, at about 11. Notably, all but 1 of the 7 patients with ADAS-cog12>=20 had cognitive decline (higher ADAS-cog12) at 3 months. Such patients are likely more representative of what to expect from the phase 3 trial.
ADAS-Cog12 change at 3 months (BIVI company presentation)
{kind=link}
As highlighted by the table below patients enrolled in the phase 2 study had by far milder cognitive impairment compared to patients enrolled in the phase 3 study.
| Phase 2 study |
| Phase 3 study |
| Number of patients |
| 23 |
| 400 |
| AD severity (inclusion criteria) |
| MCI/mild (CDR 0.5-1, 78% had CDR 0.5) |
| Mild to moderate (CDR 1-2) |
| Mean baseline ADAS-Cog12 |
| About 15 overall, about 11 in MCI/mild patients* |
| 28 |
| Mean baseline MMSE |
| About 24 overall, about 27 in MCI/mild patients* |
| 20 |
* Estimated from the relevant figures .
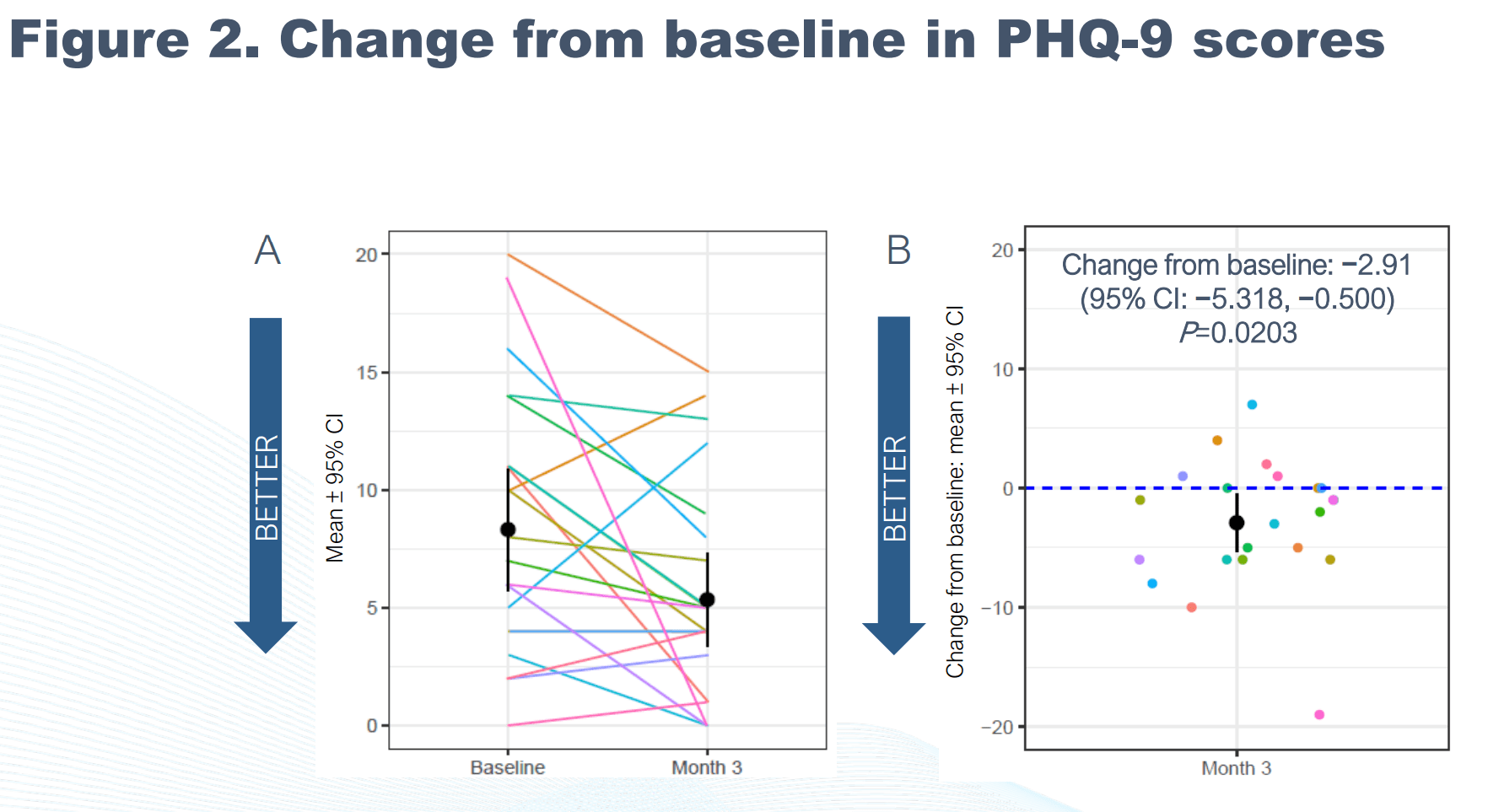
Of interest also is a presentation by BIVI on effect of NE3107 on depression. According to the presentation 68% of enrolled patients in the phase 2 study had a PHQ-9 score>=5 (indicative of mild, moderate, or severe depression). Based on Figure 2 (see below) of the same presentation 6 patients had PHQ-9 score 10-14 (moderate depression), 2 patients had scores in the range of moderately-severe depression and 1 patients had a score of 20 (severe depression). Based on the same Figure, PHQ-9 improved by a mean of -2.91 during the study, while many patients had much more dramatic improvement. The reason I am mentioning all these is because depression is a reversible cause of cognitive impairment and among exclusion criteria of the phase 2 study is: "Reversible causes of cognitive impairment that explains the clinical status entirely, such as hypothyroidism, depression". Assessing the causality here is difficult, given the lack of a placebo control. Did NE3107 through its anti-inflammatory action improve both AD and depression? Possibly. However, it is also possible that patients' cognitive impairment was partly explained by depression and by improving depression cognition followed.
PHQ-9 (depression scale) change at 3 months (presentation on 78th Annual Scientific Convention of the Society of Biological Psychiatry)
{kind=link}
AD phase 2 trial results; Placebo effect or real drug effect?
As described above, the phase 2 study was not placebo controlled. Therefore, the extent to which observed improvement was attributable to treatment vs placebo effect or other standard of care interventions is unclear. Notably, patients with MCI (majority of patients in the study) may never progress to AD and up to 16% may even revert to normal cognition.
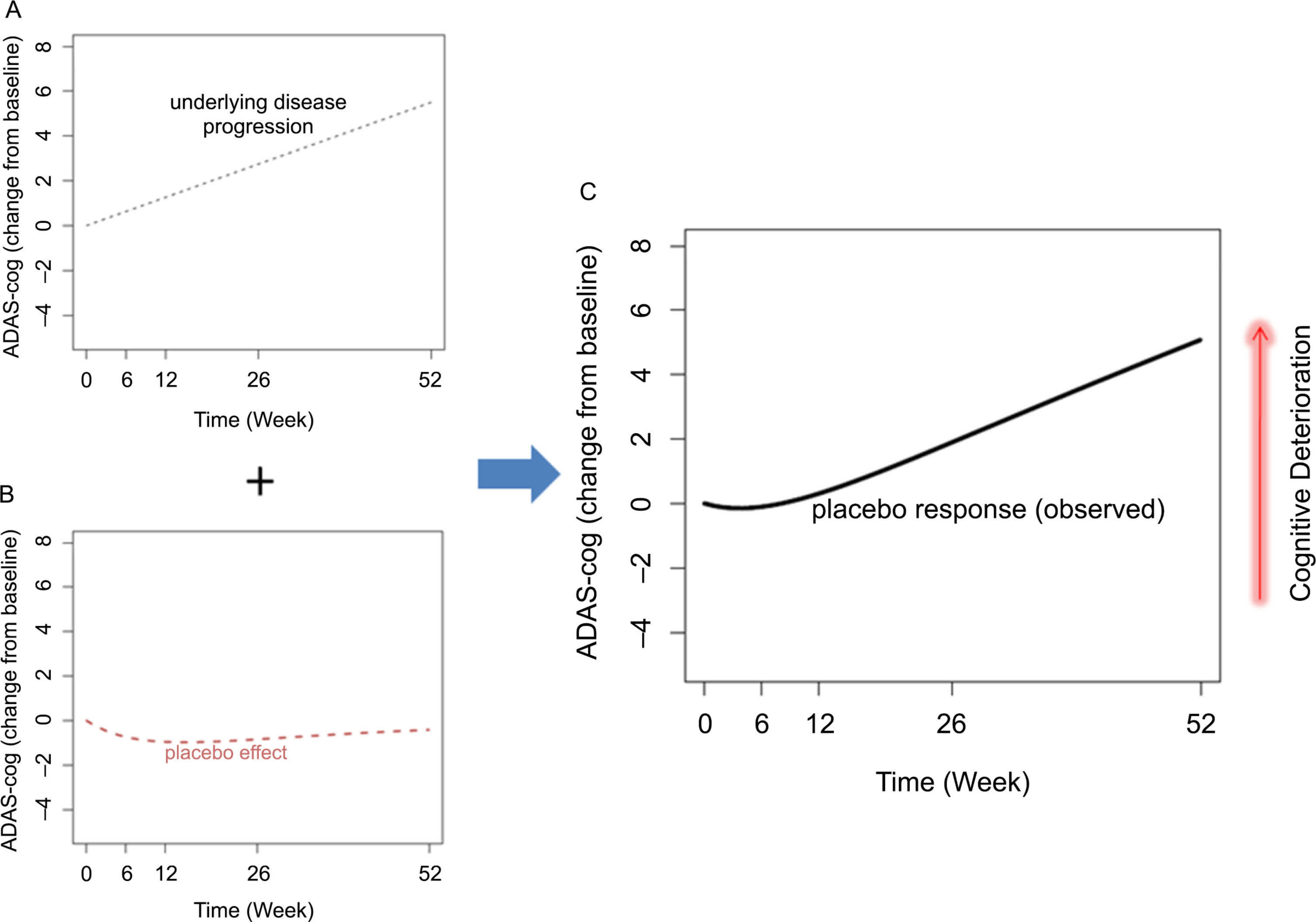
With regards to placebo effects it is important to know the timing of maximum placebo effect and how long it takes for this effect to wear off. According to Ito et al maximum placebo effect occurs at around 11 weeks and disappears within 1 year. Therefore, the 3 month duration in the phase 2 study was in my opinion not only too short to differentiate placebo from real drug effect, but the readout was actually done very close to the time of maximum expected placebo effect. Thus, it is difficult to conclude to what extent the reported effect was real or result of the placebo effect. Even the 7-month (6 month post-titration) duration chosen for the phase 3 study is too short in my opinion, as evident by durations used in other AD phase 3 trials (12-18 months). To my undersanding BIVI is hoping that at 7 months results will be much better than at 3 months, however this assumption does not account for the either the placebo effect described above or the much worse baseline cognitive impairment in phase 3.
Placebo effect in subjects with cognitive impairment (doi: 10.1016/bs.irn.2020.03.032)
{kind=link}
On the other hand, improvements in various i maging and inflammatory/AD biomarkers as well reduction of DNA methylation were observed in the phase 2 study. Importantly, such changes in biomarkers were correlated with improvements in cognition. These findings suggest a real treatment effect, rather than just placebo effect (it is unlikely that placebo could have affected biomarker data). Furthermore, the level of consistent improvement observed in multiple cognitive scale is not to be expected in AD patients without treatment.
Why I believe the current phase 3 study will fail to meet the primary endpoint
To sum up above-discussed considerations;
BIVI has proceeded to a phase 3 trial with very limited de-risking by phase 2 data. A single phase 2 study has been conducted, which was too small (n=23 patients) and too short (3 months). Given the short study duration, at least some of the reported efficacy may be attributed to placebo effect. Furthermore, phase 2 study patients had much milder cognitive impairment compared to the phase 3 study (MCI/mild AD in phase 2 vs mild-to-moderate AD in phase 3). Notably, phase 2 study patients with higher baseline cognitive impairment did not do as well as implied by the mean ADAS-Cog change. Therefore, treatment effect in phase 3 trial will be much worse than reported effect in phase 2 trial. Finally, phase 3 study is much smaller and much shorter (possibly insufficient to allow enough seperation between placebo and treatment) compared to prior AD phase 3 studies.
All above factors in my opinion increase the risk that the phase 3 trial will miss its primary endpoint. Much worse baseline cognitive impairement combined with relatively small study size and relatively short study durarion all point that the phase 3 trial might be underpowered. Therefore, I view the phase 3 study as a larger than necessary phase 2 study that will provide useful insight for planned phase 3 studies. There could still be (and likely will be) promising signals of efficacy but market is usually unforgiving to non-significant p values or worse than anticipated efficacy (see SAVA example).
Notably, BIVI's stock price (and market cap) has been steadily declining instead of rising towards the phase 3 topline results, probably reflecting markets expectations on phase 3 topline results. BIVI has at the time of writing an Enterpise Value of just about $107M .
Financials
Based on Q1 report BIVI had cash and cash equivalents of about $31.3M as of March 31, 2023, $44M including "investments in U.S. treasury bills" and "prepaid and other assets". R&D expenses were $11.2M and G&A expenses were $2.5M. At this burn rate BIVI's cash should barely be enough for about 2-3 quarters (Q2-Q4 2024). However, operating expenses will most likely increase significantly considering BIVI's plans to initiate six phase 3 trials in the next 4 quarters.
Risks to the thesis
The obvious risk to my thesis is that BIVI might prove me wrong and announce positive (statistically significant) results in October/November. Despite above-discussed limitations, the phase 2 trial has shown consistent improvement in multiple cognition scales (better that what would be expected for placebo effect), improvement in multiple biomarkers and correlation between improved biomarkers and improved cognition, all pointing to a real drug effect than just placebo effect.
My thesis also assumes a significant fall in the stock price after topline results in October/November. However, markets are unpredictable, and signals of efficacy overall or in subgroup analyses (e.g. in mild patients) may be viewed as positive considering planned phase 3 trials.
Another risk to the thesis is the potential for partnership announcement for any of the ongoing clinical programs. However, this seems unlikely before topline AD phase 3 results.
Recommendation
Overall, I tend to be bullish on BIVI long-term. BIVI is very undervalued if successful in any of the 3 current targeted indications, of which I am especially bullish on ascites indication (based on de-risking by very promising phase 2b results). However, AD is the largest indication and there is in my opinion a high likelihood that the phase 3 trial (topline results in October/November) will fail to meet the primary endpoint, resulting in a big hit in BIVI's stock price and need to raise cash from a dismal financial position. Therefore, my plan is to re-evaluate after topline results. More aggressive investors may prefer to hold through topline results and average down in case of a dip following negative results (assuming positive signals from the phase 3).
For further details see:
BioVie Pharma; Bullish Long-Term But Bearish On Upcoming Phase 3 Readout