BIVI - BioVie: Upcoming Phase 3 Readout In Alzheimer's May Create Significant Value
2023-11-15 18:54:16 ET
Summary
- BioVie is set to report topline data from its Phase 3 trial in Alzheimer's disease, with a high likelihood of reaching statistical significance.
- Blinded data from the trial showed a reduction in amyloid burden and cognitive improvements in about 75% of patients.
- NE3107, BioVie's drug candidate, appears to show efficacy across all hallmarks of Alzheimer's disease, including aging.
- Though full data have not been communicated, my analysis of the blinded data indicates a high likelihood of reaching statistical significance.
- BioVie, trading at a $120 million market cap, may see significant upside in case of positive results.
Thesis
BioVie (BIVI), currently valued by the market at about $120 million, is about to report topline data from a Phase 3 study in Alzheimer’s disease [AD] between Thanksgiving and early December. In my previous coverage , I had argued that the baseline data in about 75% of patients of its Phase 3 trial had already de-risked the possibility that patients on trial would not see a treatment effect. The current coverage provides my insights into the blinded data presented by BioVie at CTAD 2023.
At CTAD 2023, BioVie presented blinded Phase 3 data in about 75% of patients from its Phase 3 trial. An estimated 71% of patients who were amyloid-positive when they enrolled became amyloid-negative after six months of NE3107 treatment. This unexpected result added to the aging-related evidence that had been generated already, including a reduction of the biological clock by 3.3 years over 3 months.
The blinded data showed consistent and strong cognitive improvements over baseline on all 7 measured rating scales. Those effects are in line with cognitive stabilization and/or improvements on different rating scales as reported from a shorter open label Phase 2 trial earlier this year. BioVie has considered that the scattering of data and consistency of the measurements are indicators of a potential treatment effect. Meta analyses however show that the results, even blinded, are well outside historical trial and placebo values. My probability analysis for the Adas-Cog cognitive rating scale on the basis of the blinded data indicates that chances of these results being solely due to placebo are unlikely, and chances of reaching statistical significance are high.
If correct, NE3107 may significantly outperform results generated by big pharma’s anti-amyloid antibodies to date, and may be the first of the treatments focused on inflammation and metabolic dysfunction to report success in a placebo-controlled trial.
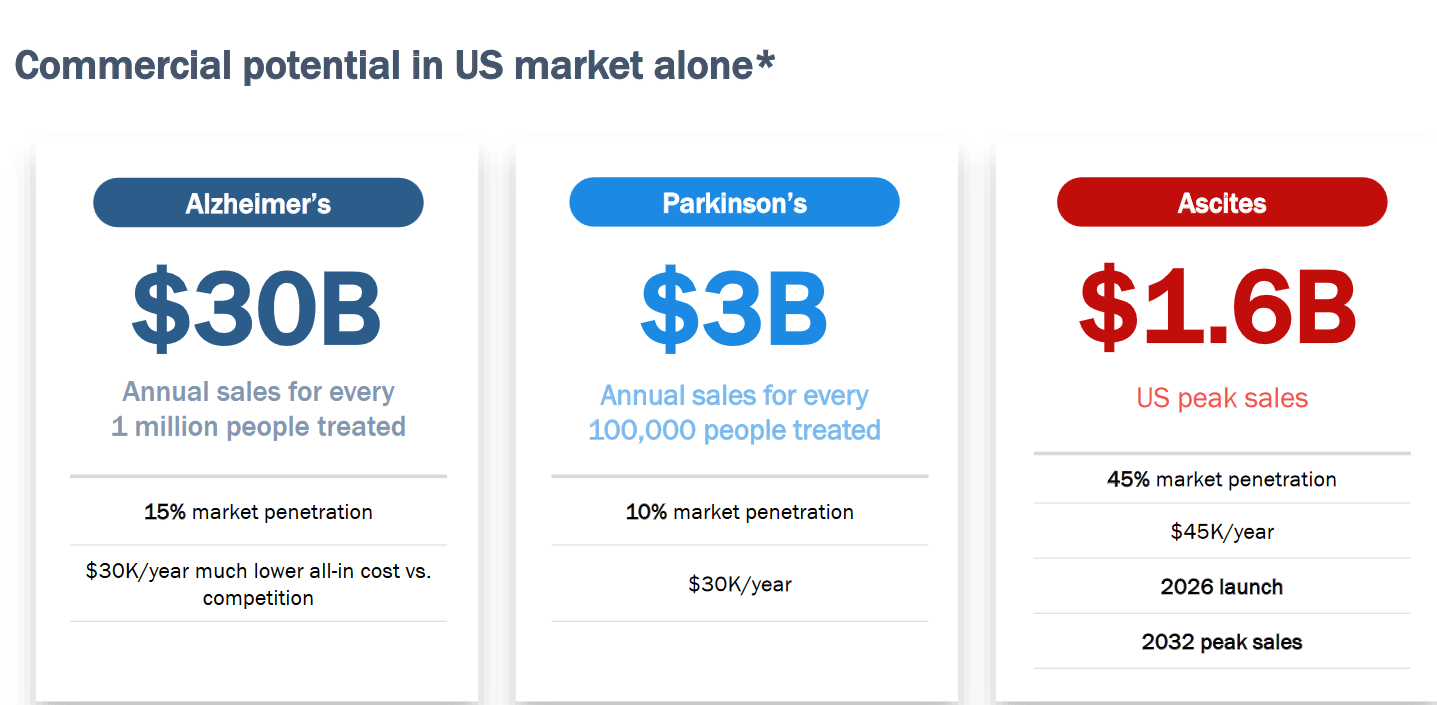
The totality of the biomarker and cognitive data and the CEO’s palpable optimism indicate to me BioVie may be expecting a positive readout. As a disease-modifying drug candidate, NE3107 apparently affects three major hallmarks of the disease. The stakes are high, in light of a $30 billion annual sales estimate in case of 15% market penetration, and historical multi-billion gains in case of positive Alzheimer’s Phase 3 results.
The company
BioVie is a biotech company focused on the treatment of AD, Parkinson’s disease [PD] and refractory liver ascites. BioVie’s drug NE3107 is an anti-inflammatory insulin-sensitizer that BioVie intends to bring to market in AD and PD. The company also has BIV201 in its portfolio which is a de-risked treatment candidate to improve the lives of patients suffering from liver ascites. Its market cap at the time of writing is about $120 million. This is its stock chart over the past year.
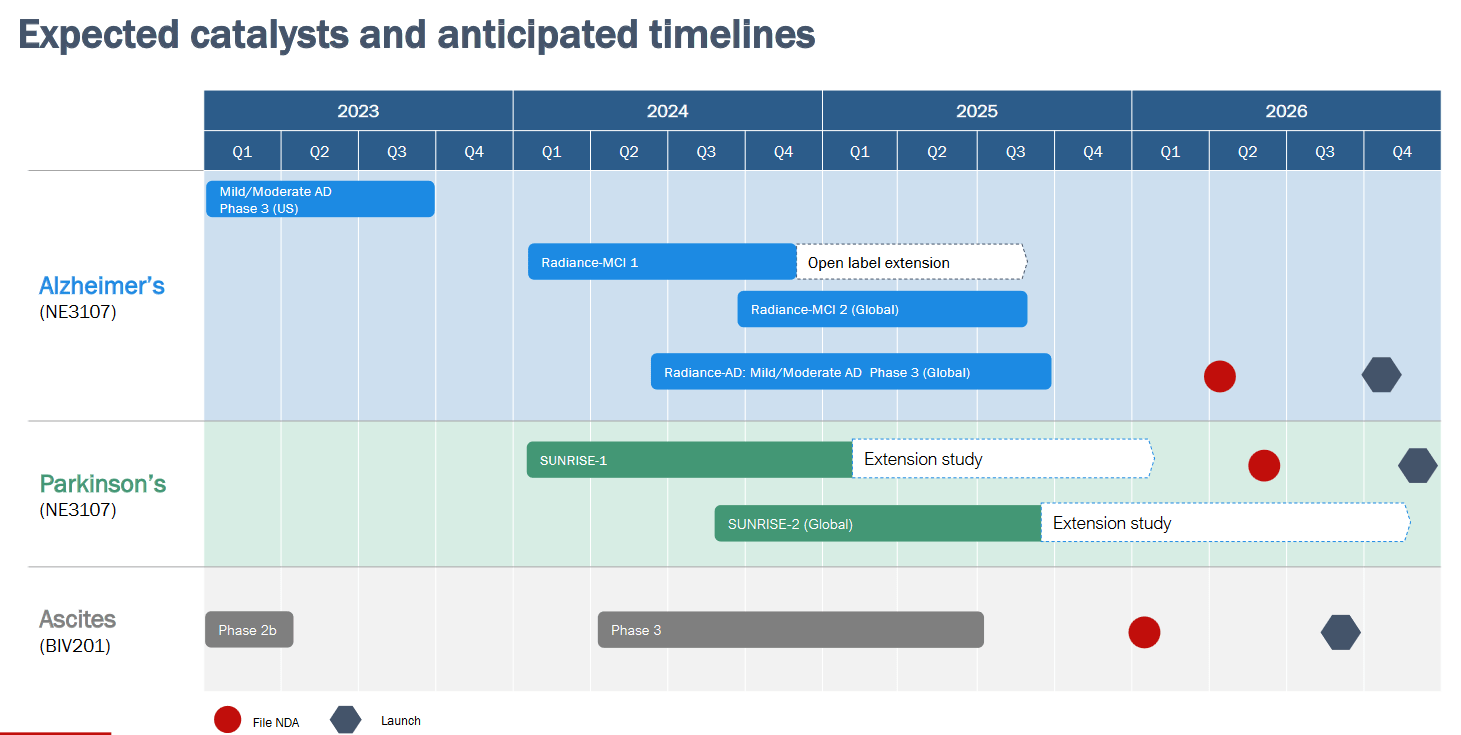
My initial coverage was part of an effort to cover the AD space. I have seen the company’s efforts in AD , PD and refractory ascites come to fruition over the past year. This is BioVie’s slide for expected catalysts and anticipated timelines.
Expected catalysts and timeline (Corporate Presentation)
{kind=link}
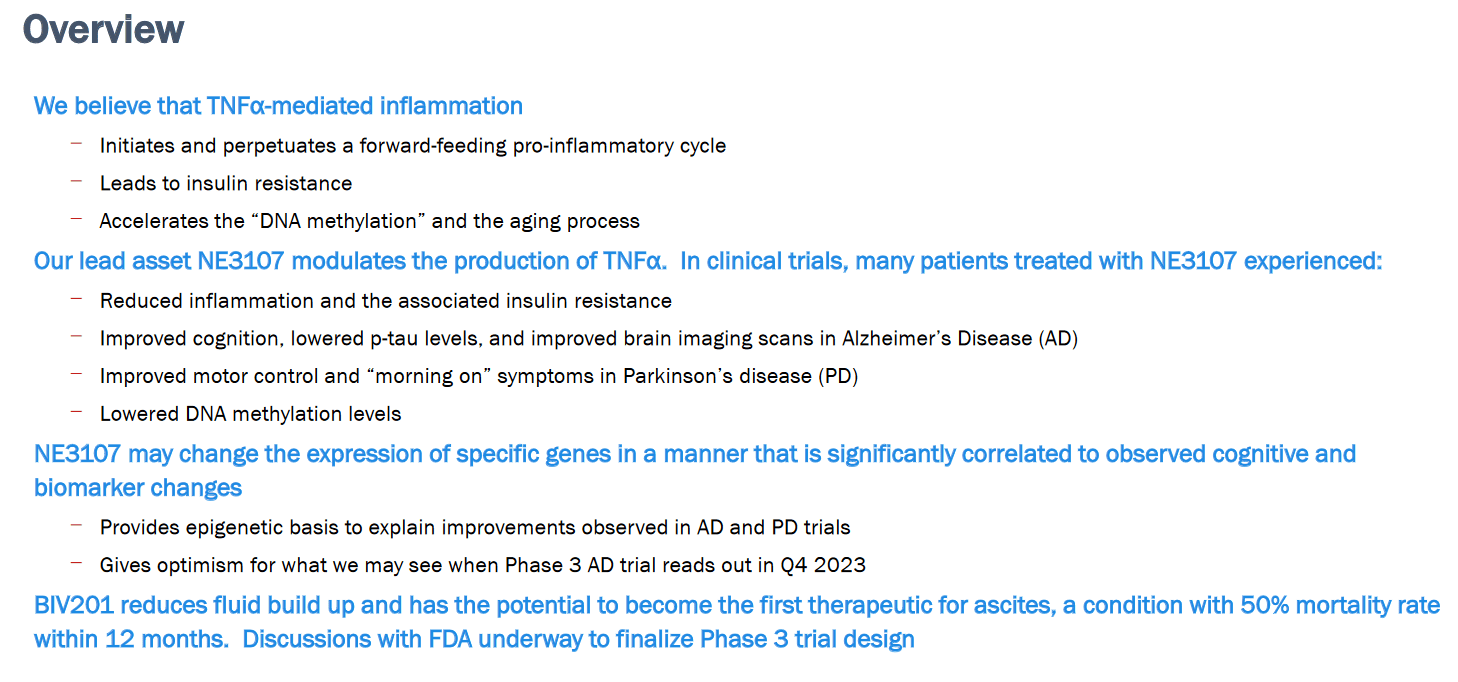
BioVie’s current corporate presentation includes the following explanatory slide on both drug candidates.
NE3017 and BIV201 explanatory slide (Corporate Presentation)
{kind=link}
NE3107 for Alzheimer’s disease
Introduction
AD is by far the largest indication BioVie is targeting with the anti-inflammatory insulin-sensitizer NE3107 . The rationale for the Phase 3 trial explains how selective reduction of inflammation and insulin-sensitization could impact two major pathways involved in several neurodegenerative diseases.
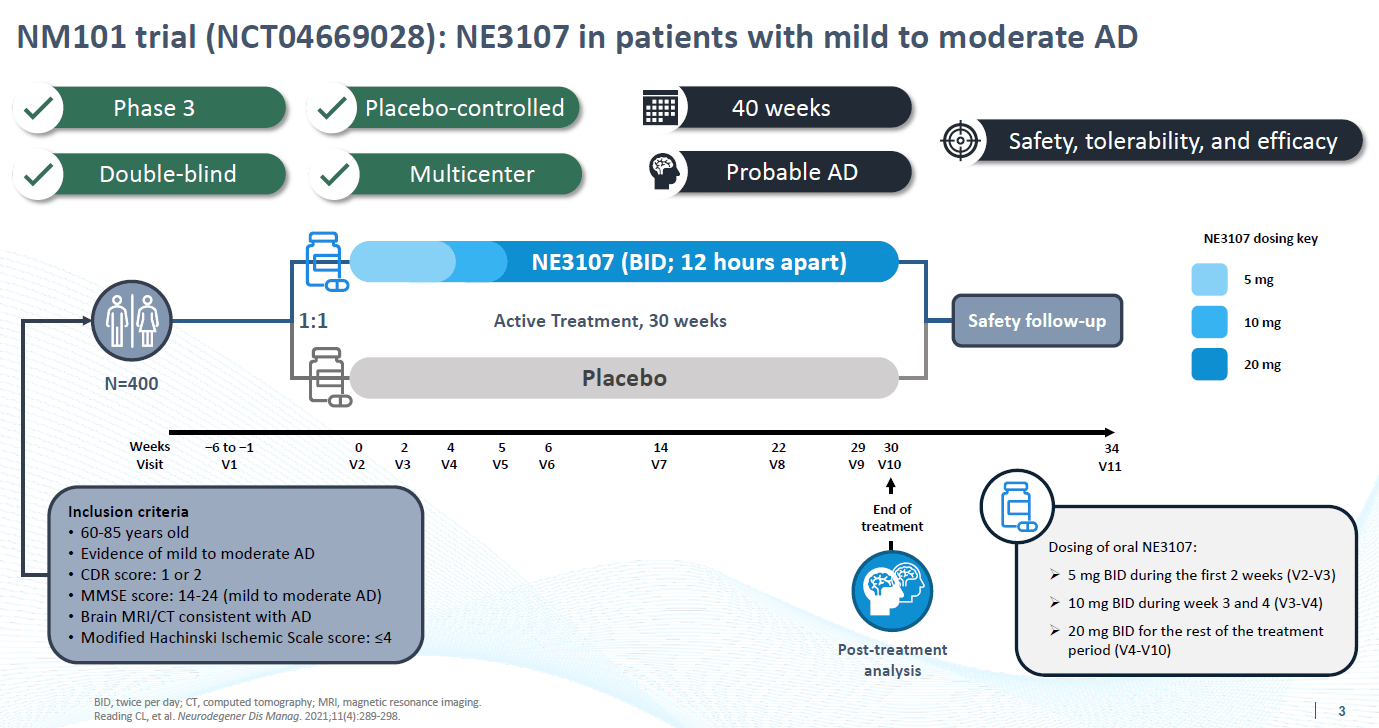
The 30-week Phase 3 trial has enrolled 439 patients and randomly assigned treated and placebo patients 1:1. Assuming a withdrawal rate of 20%, it was powered to detect efficacy and statistical significance if 125 subjects per group would be able to show a 2.5 point interval on the ADAS-Cog12 rating scale.
Phase 3 trial design (Corporate Presentation)
{kind=link}
Oral administration and safety
In contrast to recurring ARIA-E and ARIA-H safety issues with anti-amyloid antibodies, NE3107 is orally administrated, and has consistently been found to be safe and well-tolerated.
Biomarkers including epigenetics from small Phase 2 open label study
BioVie has reported findings from a small open label Phase 2 trial in AD and a small placebo-controlled Phase 2 trial in PD, which I covered in some of my earlier coverage . The most remarkable findings for me were the data on epigenetics . Aging is the most important risk factor for AD, and epigenetic dysregulation or hypermethylation of DNA is involved both in AD and PD . BioVie presented a statistically significant - and unprecedented - reversal of the biological SkinBloodClock by 3.3 years over the course of 3 months, with correlations between epigenetic results and improvements in cognition and biomarkers.
Further reportings from the open label Phase 2 trial confirmed disease modification.
- Statistically significant reduction of CSF p-tau* levels by 5%, or -1.66 pg/mL, contrary to normal increase in tau levels by about 1.5% every 3 months.
- Statistically significant reduction of p-tau* to A?42 by -0.0024.
- Improved brain region activity in 18 of 22 patients.
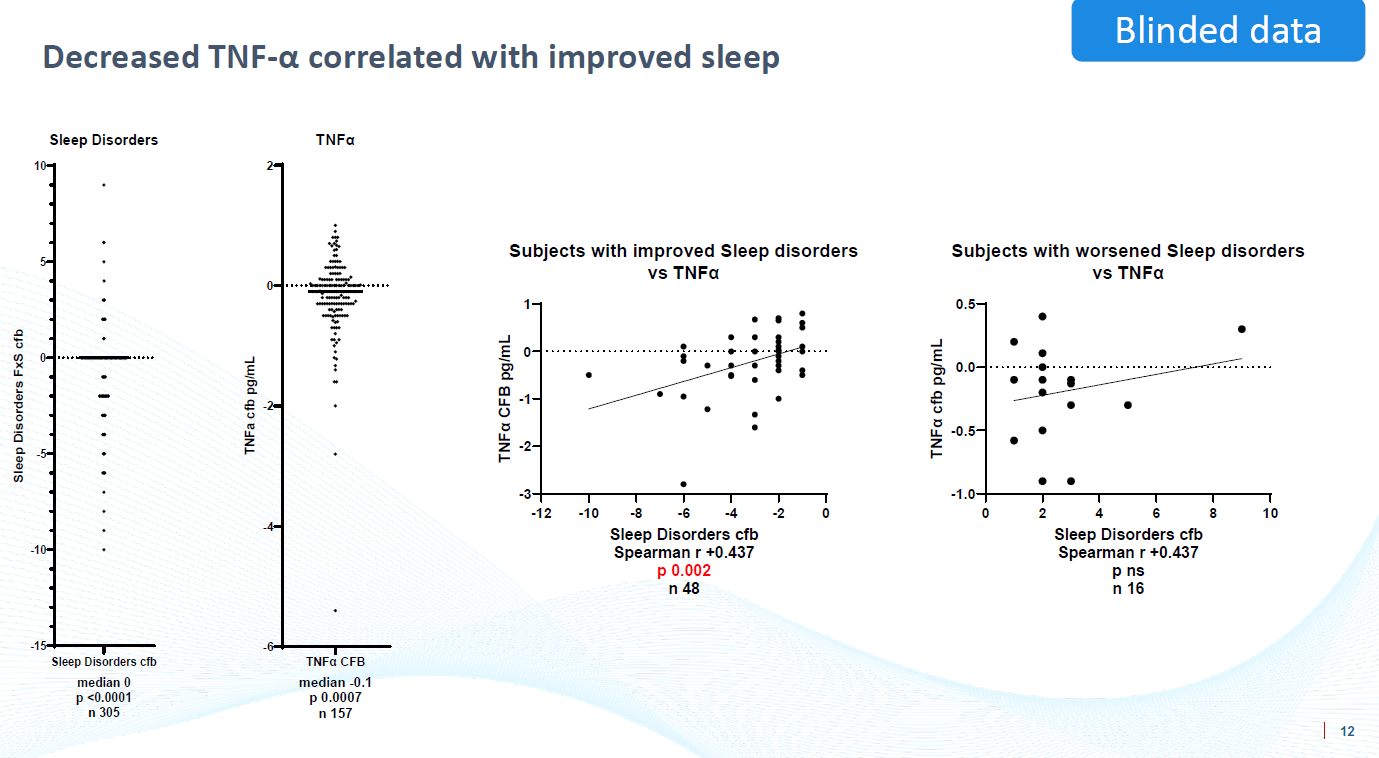
- A correlation between reduction of TNF-?** and cognitive decline.
* Neurofibrillary tau tangles are considered the second traditional hallmark of Alzheimer’s. Lowering their presence, without directly targeting tau, different to the many failed/discontinued studies with anti-tau antibodies/tau-stabilizers/aggregation inhibitors, is indicative of disease-modification.
**TNF-? is considered the master regulator of inflammation , more recently seen as a key driver of neurodegenerative diseases .
Phase 2 results on cognition
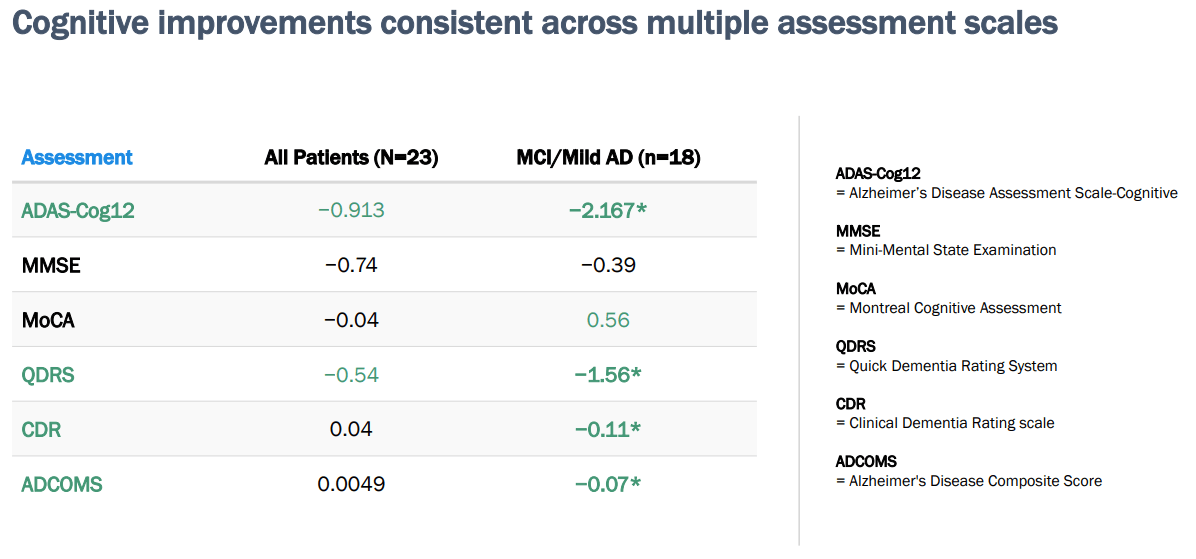
These were the results from the open label study in patients with mild cognitive impairment of mild Alzheimer’s disease. At three months, NE3107 showed improved cognition on 2 out of 6 rating scales in all patients, and on 5 out of 6 rating scales in patients with milder stages of disease.
Phase 2 results on cognition (Corporate Presentation)
{kind=link}
BioVie has also reported efficacy in a Phase 2 study in Parkinson’s disease, showing clinically meaningful improvements in patients’ motor scores, and the statistically significant finding that more patients were in the ON-state at least 8 hours after their symptomatic treatment wore off.
The Phase 2 open label study in AD was designed less stringently than BioVie’s phase 3 trial. Based on the knowledge about the patient population most likely to profit from NE3107 and BioVie’s communication of baseline data for about 75% of patients enrolled in the Phase 3 trial, I took the stance that we could see stronger efficacy in BioVie’s Phase 3 trial.
Biomarker data presented at CTAD 2023
Reduction of amyloid burden
The finding
Oligomeric amyloid buildup is a traditional yet debated hallmark of AD. About 30% of people who have brains full of amyloid do not have dementia. Chronic neuroinflammation is the possible trigger to actual development of dementia, with amyloid accumulation as one of several inflammatory triggers.
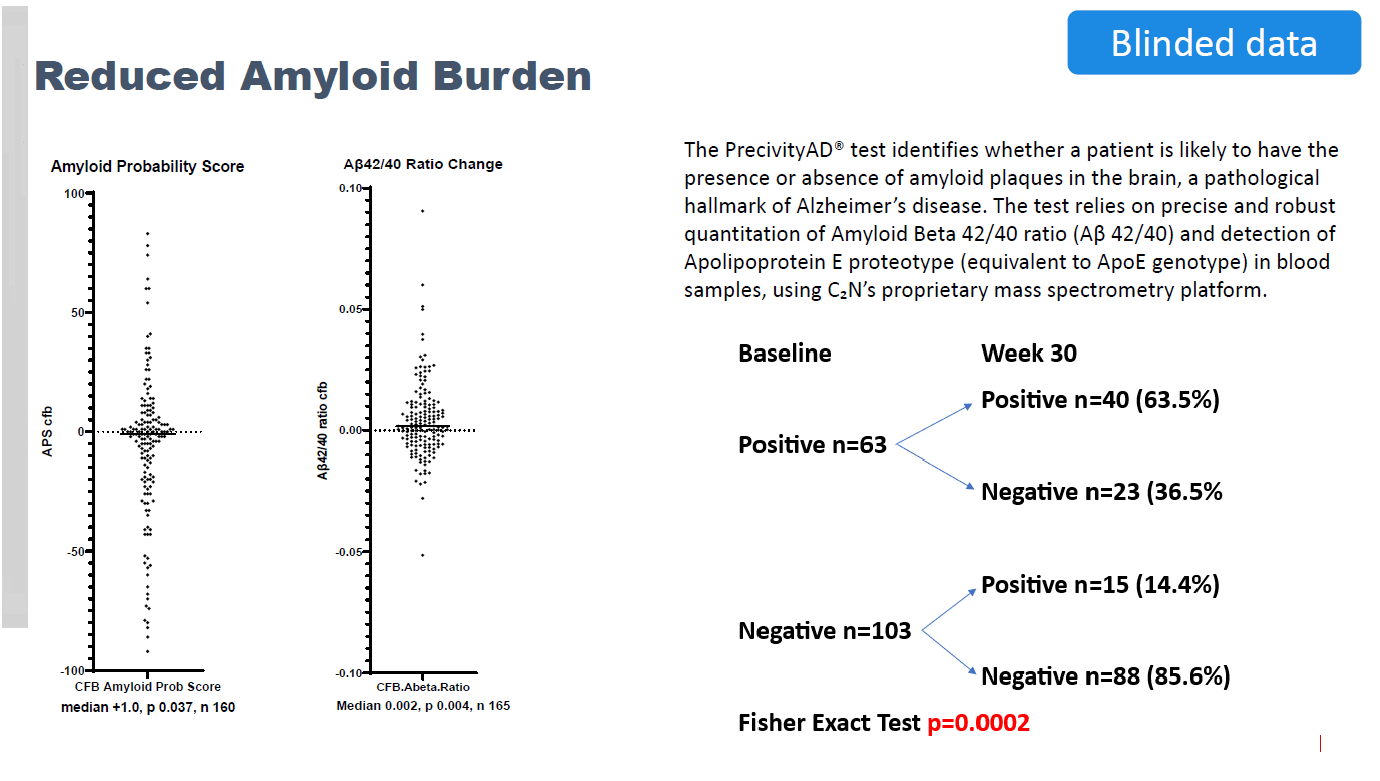
BioVie reported at CTAD that, of the 63 blinded patients who were amyloid-positive at baseline, 36.5% or 23 patients became amyloid-negative after six months. This is yet another unprecedented finding indicating disease modification, and it is one that I believe will be of particular interest for big pharma.
Reduced amyloid burden (CTAD Presentation ) Reduced amyloid burden PET substudy (Corporate Presentation)
{kind=link}
{kind=link}
The possibility of NE3107 reducing amyloid was unexpected. BioVie assumes that less TNF leads to less amyloid precursor protein and hence to lower amyloid burden. In a KOL webinar , BioVie considered the possibility that better- phagocytosing glial cells may be implicated too. NE3107 may trigger naturally correcting biological mechanisms in those with an amyloid burden. If there was an equal distribution of amyloid-positive patients across placebo and NE3107-treated patients, 73% of patients would be relieved of their amyloid burden after six months.
Comparison with FDA-approved anti-amyloid antibodies
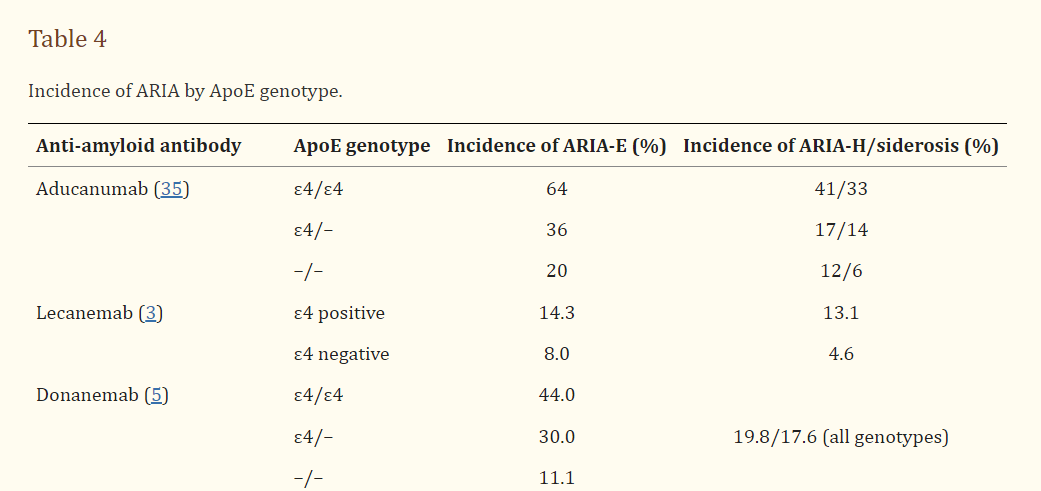
Biogen’s ( BIIB ) Aduhelm received accelerated approved due to its A?-lowering effects by respectively 59 and 71 percent over 18 months, without showing cognitive efficacy. An extrapolation to six months could imply Aduhelm reduces A? by 20 and 23 percent. Additionally, Aduhelm reduced the second traditional hallmark of AD, neurofibrillary tangles of phosphorylated tau, showing a 13-16% reduction of biomarker p-tau181 % over 18 months, or 2.17-2.67% over three months. Anti-amyloid antibodies come with a safety warning . Their side effects, ARIA-E and ARIA-H , are mostly present in AD patients with the highest risk factors for AD, namely APOE4-gene carriers. APOE4-homozygotes have a 9-15 times higher risk of developing AD, and with heterozygotes that risk is 3-4 times higher. Brain amyloid plaque loads are higher in APOE4 carriers. The safety risk of anti-amyloid antibodies in exactly those patients, with substantially higher chances of developing AD, is much higher.
Biogen (BIIB)/Eisai’s ( OTCPK:ESALF ) ( OTCPK:ESAIY ) antibody Leqembi, FDA-approved in 2023 for MCI and mild AD, led to reduction of brain amyloid in two thirds of amyloid-positive patients after 18 months.
ARIA incidence by APOE genotype (Front. Neur. 2022, Amyloid-Related Imaging Abnormalities With Anti-amyloid Antibodies for the Treatment of Dementia Due to Alzheimer's Disease)
{kind=link}
Some anti-amyloid antibodies such as Roche’s ( OTCQX:RHHBF , OTCQX:RHHBY , OTCPK:RHHVF ) crenezumab were not successful in lowering amyloid burden. Roche’s failed gantenerumab took two years to clear amyloid burden.
NE3107 appears to reduce amyloid burden without side effects in 73% of amyloid-positive patients over only six months’ time, in a harder to treat mild and moderate AD population, without directly targeting amyloid burden, and without side effects. NE3107 has shown a 5% reduction of p-tau181 over 3 months. If NE3107 were to confirm these findings upon unblinding, NE3107 could address the three well-established targets of Alzheimer’s disease, amyloid, tau and neuroinflammation without safety issues. If confirmed, I believe those findings may open up a pathway of accelerated approval for NE3107, which BioVie touched upon during the latest KOL webinar , which could raise chances for future successful commercialization.
Further biomarkers and correlations
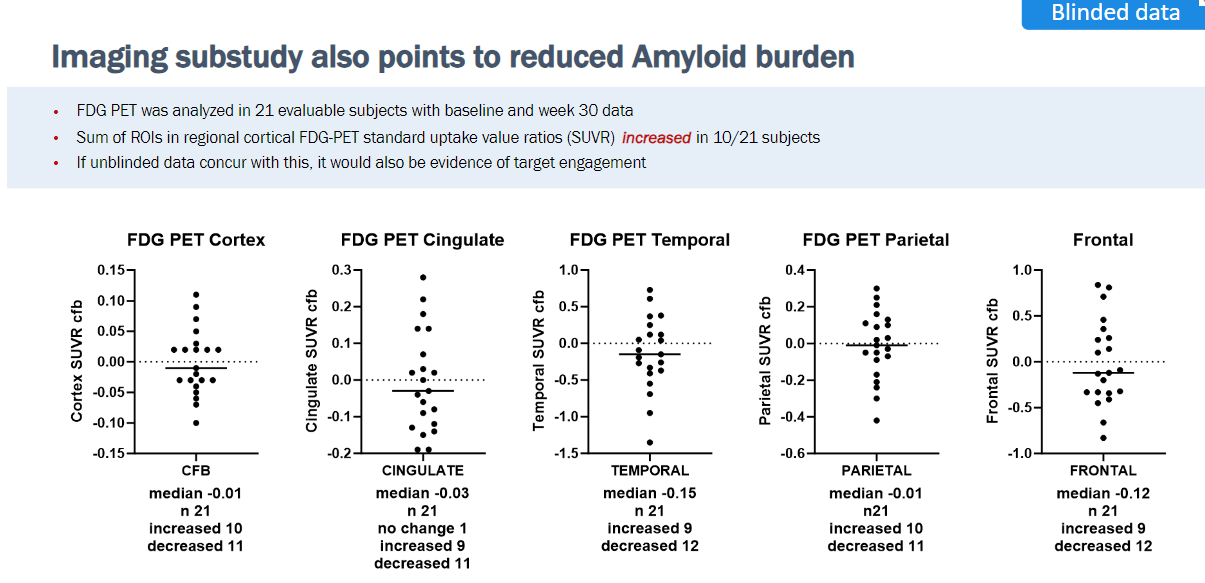
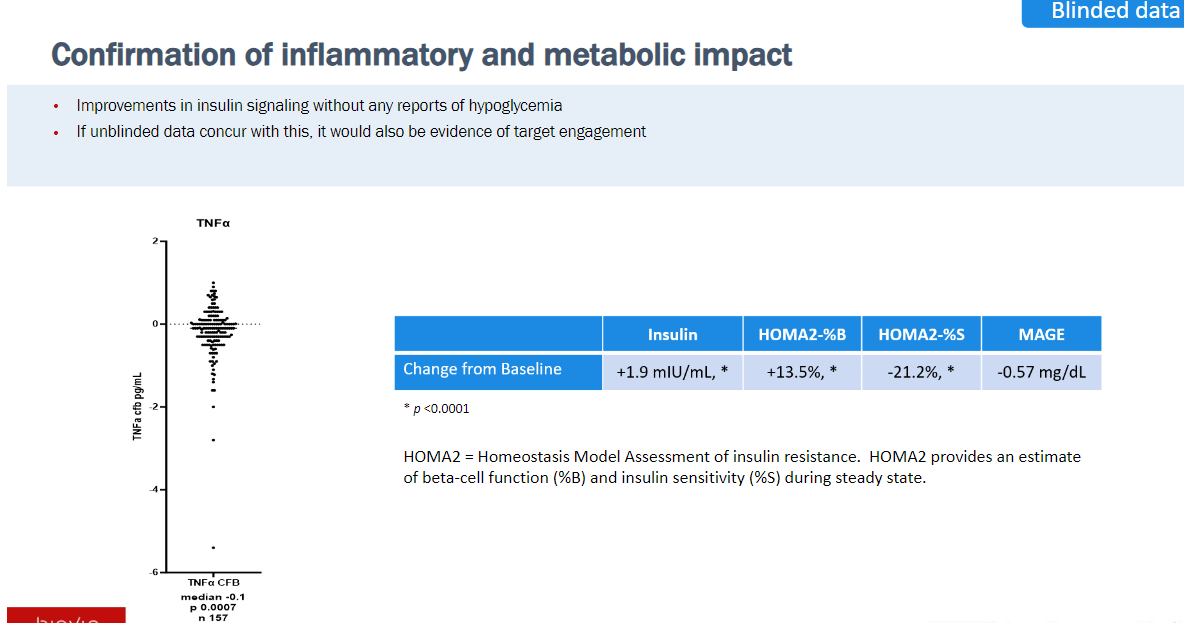
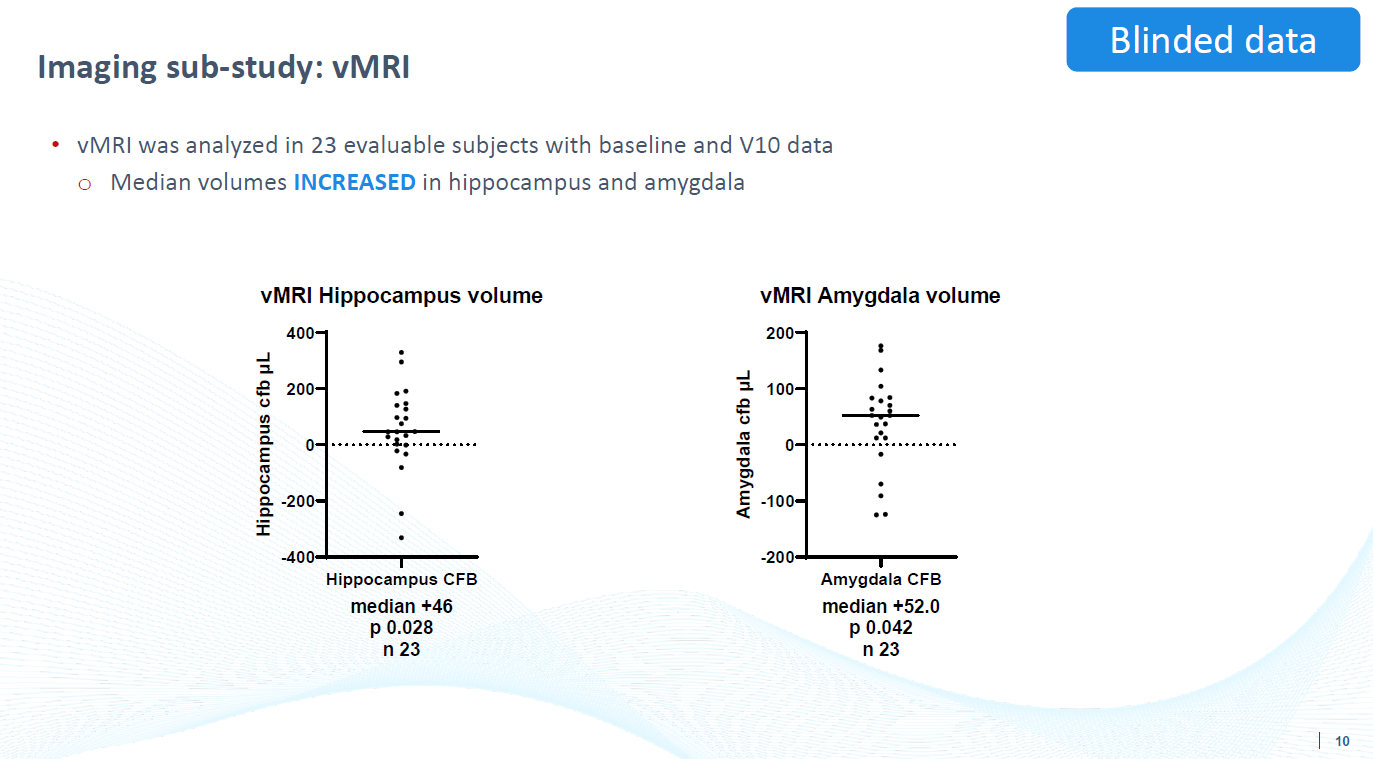
BioVie further reported reduction of TNF, correlation between reduction of TNF and improved sleep, reductions of biomarkers FDG-PET and volumetric MRI in a subset of patients, increases in insulin and beta cell function without hypoglycemia.
Insulin signaling improvement (CTAD presentation) TNF correlation with improved sleep (CTAD presentation) vMRI slide (CTAD presentation)
{kind=link}
{kind=link}
{kind=link}
Further biomarker data may be announced when topline data is released or – more likely – later, probably around January 2024. I am particularly interested in data on NfL and p-tau.
Blinded cognition data presented at CTAD 2023
Consistent cognitive improvements
At CTAD 2023, BioVie presented blinded data on 322 patients that were available for analysis as of October 18, 2023, followed by a press release and a KOL webinar on November 1, 2023. For the record, about a quarter of the patients are still missing.
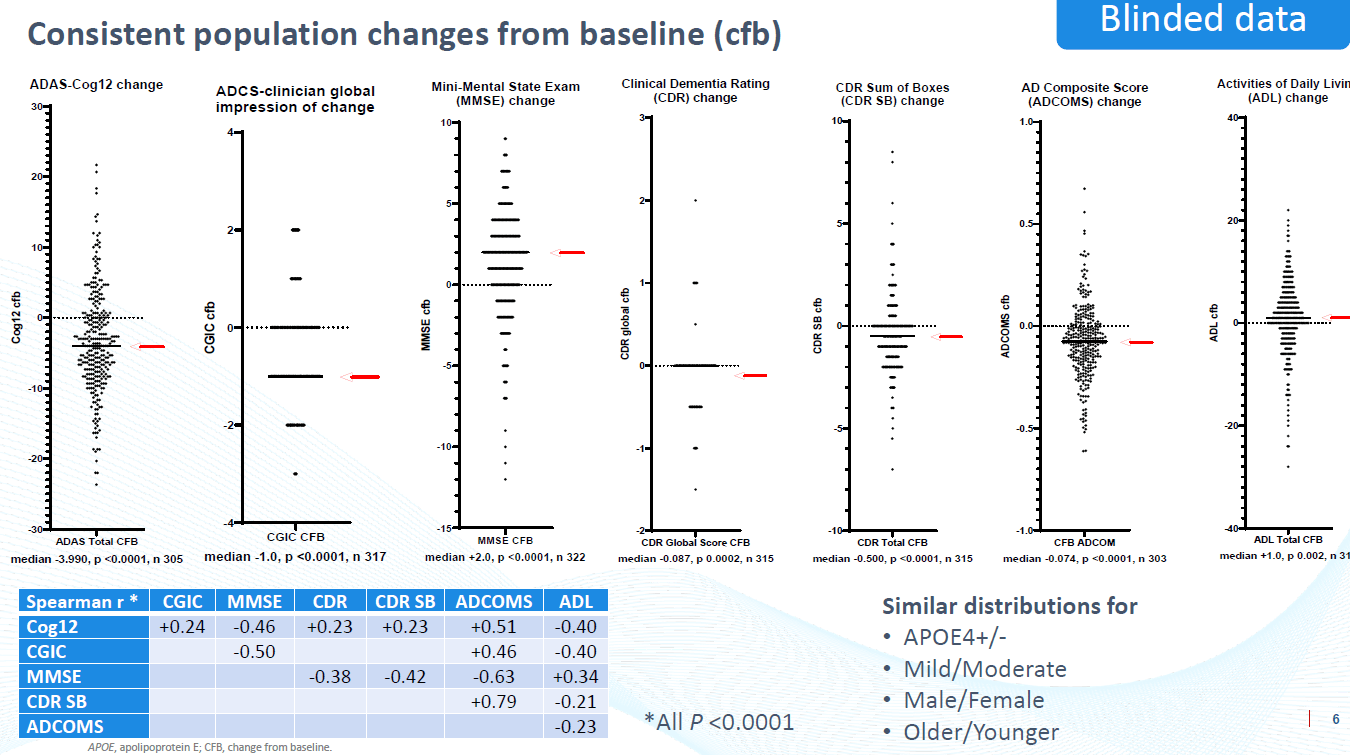
BioVie reported statistically significant population changes from baseline for all primary and secondary cognitive and functional assessments measured: ADAS-Cog12, ADCS-CGIC, MMSE, CDR, CDR-SB, ADCOMS, and ADL. In other words, the blinded data in about 75% of all patients saw an improvement of cognition, across all measured rating scales, with similar distributions across subgroups APOE4/-, mild/moderate, male/female, older/younger.
Cognitive improvements slide (CTAD presentation)
{kind=link}
BioVie has stated that the scattering of the cognitive data is the main takeaway here, as the data would be more clumped together if no drug effect would be seen. During a subsequent KOL webinar , BioVie added that it seems implausible that such data would come from placebo alone, given the consistency and strength of blinded results together with biomarkers.
Comparison with standard trajectories
The blinded cognitive results are remarkable and raise the question whether BioVie’s trial could not be suffering from a placebo/learning effect. One cannot exclude such an effect, but it appears likely that treated patients nonetheless outperform placebo patients in a statistically significant manner.
I consider CDR-SB, MMSE and Adas-Cog the most relevant rating scales, as they are used most frequently.
These can be considered normal AD trajectories on the MMSE, CDR-SB and Adas-Cog[13] rating scales.
Normal decline Adas-Cog, CDR-SB, MMSE (Finding Treatment Effects in Alzheimer Trials in the Face of Disease Progression Heterogeneity)
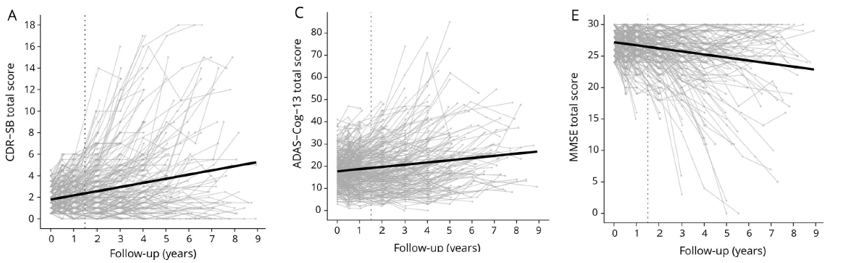{kind=link}
The average rates of cognitive decline for MMSE , CDR-SB and Adas-Cog11 [not Adas-Cog12], extrapolated to a period of six months, show the following average normal decline.
Average normal decline (Own work)
The BioVie blinded data in about 75% of patients are as follows [estimates].
Improvement, unblinded (Own work)
The difference between average normal progression and average decline, unblinded, would then be as follows.
Difference normal progression and average decline, blinded (Own work)
The exercise would be similar for all seven measured rating scales, as all showed improvement. Note the 6.75 interval for Adas-Cog, focus of the analysis below.
If confirmed, the market reaction could be tremendous. The threshold for success for a disease-modifying drug in AD is about 27-35% slowing of cognitive decline, as confirmed by BioVie. The 27% slowing of decline was generated by Leqembi. Donanemab, yet to be approved, showed a 36% slowing of cognitive decline. For reference, when Biogen/Eisai reported topline data for their anti-amyloid antibody Leqembi, market reactions of $2 billion, $11 billion, $11 billion and $22 billion were seen for respectively Eisai, Biogen, Roche and Eli Lilly.
Likelihood of a treatment effect
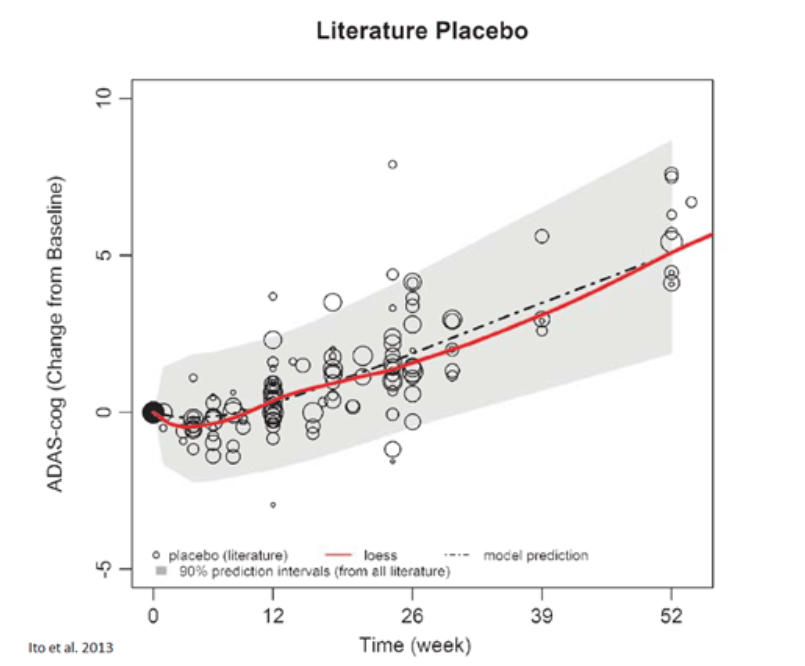
If there would be a placebo/learning effect, the question is how strong it could be. A meta-analysis of placebo response of mild to moderate AD patients on the Adas-Cog rating scale shows the expected cognitive decline over time within a 90% prediction interval. A follow-up study of placebo patients showed a normal disease progression of 5.82 points per year, with very few and outlying studies showing results close to BioVie’s reporting of -4 points, blinded, for the record.
Meta analysis Adas-Cog (Neurology, Disease progression meta-analysis model in Alzheimer's disease) Second meta analysis Adas-Cog (Alzheimer's Research & Therapy)
{kind=link}
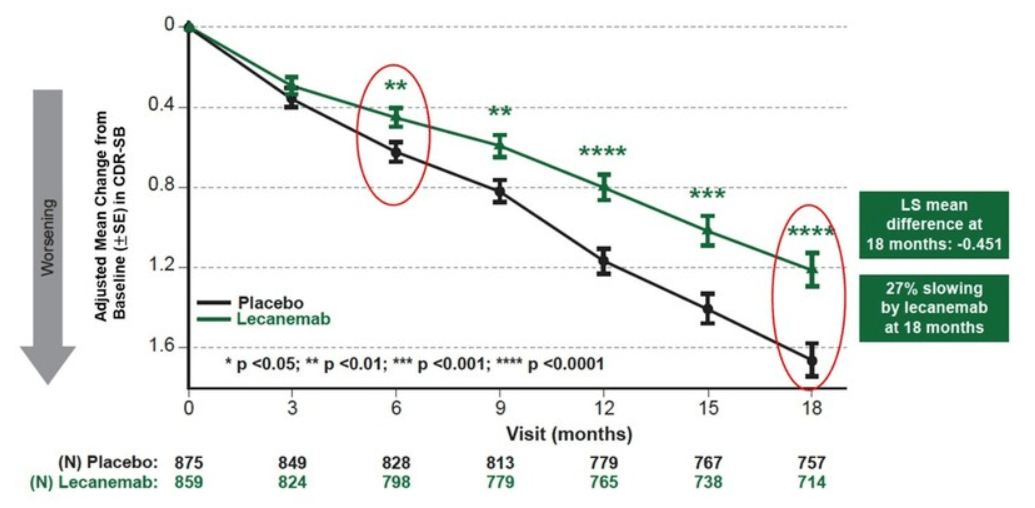
For CDR-SB, direct comparisons with the latest two positive Phase 3 results from big pharma could be a reference to start with. These are the CDR-SB data for Leqembi and donanemab .
Leqembi CDR-SB slide (Biogen website) Donanemab CDR-SB slide (AAIC 2023 presentation Eli Lilly)
{kind=link}
For Leqembi, about a +0.6 point decline is shown after six months on placebo, which is 0.3 points less than historical decline, meaning one could account for a placebo effect of 0.3 points. For donanemab, about a +0.8 point decline is shown after 30 weeks, which is 0.1 point less than historical decline, meaning there is almost no placebo effect.
I conclude that BioVie’s blinded results, consistently over 7 rating scales:
- go opposite the trajectory of normal progression in AD;
- are well outside normal historical values placebo response.
These conclusions do not mean that BioVie may not be seeing a placebo or learning effect. However, it is unlikely that the blinded data would solely be due to such an effect, as I will explain below.
Likelihood of statistical significance
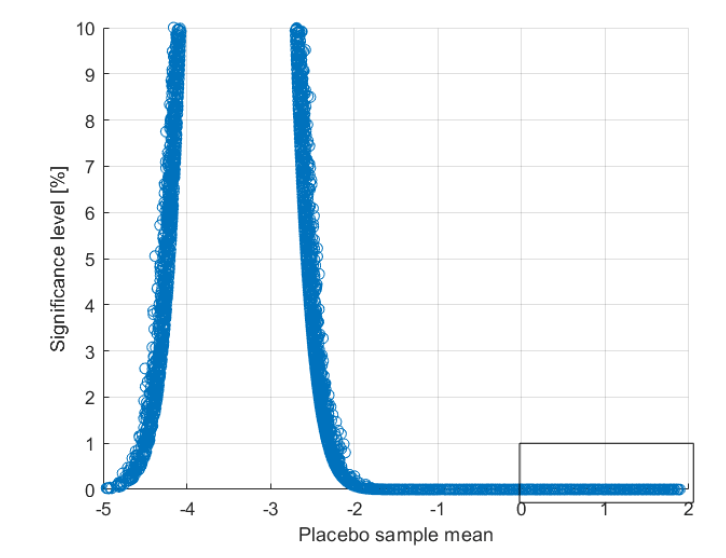
Based on the blinded Adas-Cog data points, sample distributions were created where half of the data points are always attributed to the placebo group. For each of the 143207 sample distributions created, the mean of the placebo group and the treated group were calculated. The figure below shows the statistical significance level, plotted against the mean of the placebo group. It is logical, that with an increasing improvement of the placebo group, the mean of the placebo group and the treated group become more similar.
Significance level test (Own work)
{kind=link}
My conclusion from that exercise is that, insofar as placebo patients would not have improved by -2 points on Adas-Cog on average, which is unlikely given the historical disease progression of about +2.75 points, the results from treated patients would likely be statistically significant. To be clear, even if placebo patients’ average cognition would have somehow improved even more, the results may still come back statistically significant, but not with the same degree of likelihood. Though this has been a hypothetical exercise in about 75% of patients, on only one rating scale, it indicates that BioVie’s blinded data may be exceptionally strong. BioVie’s Phase 3 baseline data already indicated a seemingly good match with NE3107’s MoA, as I had indicated in earlier coverage.
Commercial potential
The AD drug market is worth about 6.5 billion, and is expected to reach $13.7 billion in 2030. The anti-amyloid antibodies and Medicare involvement are expected to drastically alter that playing field, with a $26,500 price tag but many indirect additional costs . Medicare spending is expected to swell by $56.5 billion per year upon the marketing of such antibodies. This is how BioVie sees its total US addressable market.
Commercial potential slide (Corporate Presentation)
{kind=link}
The market cap gains could be tremendous in case of a positive result from BioVie’s Phase 3 trial. I reminder investors that Eli Lilly had gained about 25 billion in market cap after it reported a 35% slowing of cognitive decline for donanemab. Biogen’s stock had soared 40%, adding $11 billion in market value, after reporting Leqembi’s 27% slowing of cognitive decline.
In my eyes, both BioVie’s safety, biomarker and efficacy data, perhaps even including on amyloid, may come in stronger than seen from the above therapies.
Finances
As of September 30, 2023 as mentioned in the latest quarterly report , BioVie has cash and cash equivalents of $21 million compared to $19 million the quarter before. Research and developments costs were $8.9 million and and general expenses were $1.9 million. Total operating expenses are $10.9 million, which means cash will last only about two quarters. Under a Sales Agreement with Cantor Fitzgerald, following which BioVie may issue and sell from time-to-time shares of the Company’s common stock, BioVie has sold shares for a total of $7.8 million during the previous quarter.
My previous coverage mentioned an S-3 filing for a primary offering of up to $300,000,000 in different securities and a secondary offering of up to 311,002 shares of class A common stock. The company's broad plans for further development and commercialization of NE3107 may therefore largely depend on a positive readout of its Phase 3 trial in AD.
Risks
I consider the following main risk factors, ranked in order of importance for me, to be taken into account when deciding on an investment in BioVie.
1) BioVie has an effective shelf offering for a total of up to $300 million. This of course entails a risk of dilution, although I have actually considered this before is a bullish sign of chances of a positive readout.
2) BioVie did not include about 25% of all patients on trial in the blinded data, and final results could differ from data reported at this time.
3) BioVie has reported blinded data excluding data from six trial sites , which may have committed scientific misconduct and non-compliance with good clinical practices and regulations, which has been dealt with in the statistical analysis plan. The market reaction to this information in a recent 10-Q caused a considerable market reaction. BioVie’s short interest is about 19%.
4) Terren Peizer is BioVie’s major shareholder, former CEO and former Chairman of the Board. He has been indited for his involvement in selling shares of Ontrak, a company he was the CEO of. The discussion revolves around the question whether he complied with the rules on insider trading plans. When BioVie found out, the board acted upon its fiduciary duties and accepted the resignation of Terren Peizer as Chairman of the Board. He is still a large holder. The remaining worry could be that he would start selling his shares. I believe that risk is all-in-all limited. As I mentioned before, Terren Peizer appears to be in it for the long haul , has provided additional funding when the price was close to an all-time low in 2022, has not sold stock when the stock ran to $12, and most of his shares are unregistered meaning he would have to register them first before he could start selling.
5) BioVie lacks clarity on what its primary endpoint will be. Originally the Phase 3 trial had a co-primary endpoint: Adas-Cog and CGIC. On June 1, 2023 , after first Biogen ( BIIB ) and then Eli Lilly ( LLY ) had reported successful topline data for anti-amyloid antibodies Leqembi and donanemab on the CDR-SB rating scale, BioVie had changed its primary endpoint to CDR-SB on CTG Labs - NCBI . This change has apparently not yet been confirmed by the FDA. In the November KOL conference call, BioVie indicated it had flexibility in this regard until data unblinding. My view on the basis of the above is that which endpoint will be reported may not matter much for efficacy and statistical significance. Leqembi and donanemab also saw similar efficacy across rating scales.
Conclusion
BioVie’s Phase 3 trial is expected to report topline data some time between Thanksgiving and early December 2023, and hence the time for BioVie and investors to unlock NE3107’s value could be near. The potential for market value gains is impressive in light of the below $120 million market cap BioVie currently has, the multi-billion total addressable market and historical market value changes of $11-$25 billion after recent successful Phase 3 reporting in Alzheimer’s.
NE3107 has systematically been reported to be safe and well-tolerated. The entirety of biomarkers, including epigenetics, indicate to me that Alzheimer’s patients could be seeing an effect from treatment with NE3107. The reported blinded reduction of amyloid burden could bring NE3107 into a different ballpark entirely. Contrary to anti-amyloid antibodies, the drug does not pose a more severe safety risk in those patients that carry the highest genetic risk for AD, namely carriers of one or two APOE4 genes.
The threshold for success is about a 27-35% slowing of cognitive decline. The blinded cognitive data in about 75% of patients show cognitive improvement, go opposite the normal disease trajectory, and do not appear to align with historical placebo values. Though about 25% of patients have not been included given the cut-off date, the blinded data suggest a potentially strong treatment effect. My separate analysis of the probability of reaching statistical significance on the Adas-Cog rating scale suggest that even if placebo patients would on average somehow improve at about the same rate as they would normally decline, the trial would still reach statistical significance. The biomarkers and consistency of improvements across seven measured rating scales appear to indicate the same.
If successful, BioVie could take a large step in its progression to approval of NE3107 for AD. Although an additional trial would in principle be needed to go for full approval, the entirety of biomarker data, including on amyloid burden, could allow eligibility for accelerated approval.
On the basis of the exceptional data discussed above, I have upgraded my rating on BioVie to Very Bullish.
For further details see:
BioVie: Upcoming Phase 3 Readout In Alzheimer's May Create Significant Value