BIVI - BioVie: Update Following Topline Results (Rating Downgrade)
2023-12-02 00:44:02 ET
Summary
- Misconduct issues were identified in several trial sites, leading to exclusion of majority of enrolled patients and a severely underpowered study.
- BIVI presented promising signals of efficacy but with many limitations. BIVI plans to resume enrolling within 3-6 months but will likely need more patients than originally planned.
- BIVI wants to partner NE3107 but the timing of that happening is unclear. Without a partnership BIVI will need to raise cash to support planned trials.
Thesis overview
BioVie ( BIVI ) announced topline results from its phase 3 trial in mild/moderate Alzheimer's disease [AD], which were very disappointing. My original feeling for BIVI ("bullish long-term but bearish on upcoming phase 3 readout") proved to be correct. However, I was then fooled by BIVI's blinded data presentation at CTAD conference, which created great expectations for NE3107. My thesis was based on data presented on n=322 patients showing improved cognition. Not considering the possibility of flawed data, these results supported that NE3107 not only could delay disease progression, but could even improve cognition.
However, following misconduct issues in several trial sites, much more than the 6 sites initially revealed in the latest 10Q , BIVI ended up presenting data for just n=57 patients. Obviously, the study ended up being severely underpowered, despite promising signals of efficacy in cognitive outcomes. I can't complain because buying the post-CTAD dip has been profitable for me. I am saying this, not to brag, but to clarify that what follows is not coming from an angry investor who lost money on BIVI.
Below I will discuss the misconduct issues, the timeline relevant to the CTAD presentation, and the data presented. Overall, to my disapointment, data were severely limited by exclusion of majority of enrolled patients.
Overview of misconduct issues
According to BIVI's PR and call, "Pentara reviewed the blinded data when enough patients completed the trial " (i.e. before CTAD presentation). Based on this review of the blinded data Pentara identified a "particular demographic group" as well as certain trial sites that had anomalous results (inconsistent data patterns compared to historical data, large proportions of patients improving compared to baseline, unusual data variability). Notably, all problematic sites and patients belonging to the "particular demographic group" were from a single geographic area. " Without unblinding and PK data, there was no way to identify the cause of the pattern. Thus, Pentara recommended a subgroup analysis of the identified demographic group vs. all others and anomalous sites vs. others when the study becomes unblinded ." Of note, what this "particular demographic group" was remains an enigma to me.
Also stated in the PR that " In parallel , some sites started to complete their patient-facing activities in early summer 2023 , which created the first opportunity for BioVie to start the data verification and assessment process. The process surfaced unusual data patterns and deviations from expectations ( missing data, suspected copied/pasted MRI results, etc. ), which led the Company to retain two new CROs to conduct a multi-step process that entailed quality control visits at all sites, performing source data verification (SDV) on 100% of the documents used in the clinical sites to ensure what was notated on paper during patient visits was accurately reflected in the EDC, and auditing the sites. This extensive, multi-month process concluded when the Company received the final report identifying six sites that appeared to have a large number of deviations from the study protocol and Good Clinical Practices ( GCP ).". As explained in the call, this report was received on November 6 (i.e. post-CTAD presentation) . Of note, it is surprising to me that misconduct issues were identified by CROs in only 6 sites, while Pentara identified "anomalous" data in additional 9 sites. In other words these 9 sites had passed the SDV.
As a results, 128 patients were excluded from the initially revealed 6 sites (as identified by the CROs), plus an additional 230 patients from the rest of the sites in the problematic geographic area (as identified by Pentara). Additionally, of 81 patients left (the modified Intention-to-treat -"mITT"- population), only 57 were available for the per-protocol analysis. Data presented later below are based on just these 57 patients.
BIVI presentation
Timing of identification of misconduct issues relevant to blinded data presentation
The presentation in CTAD was conducted in October 25 based on "participants whose data were available for analysis as of October 18, 2023" and sites that had passed the SDV by then. In other words the 6 sites that had not passed the SDV were not included among the blinded data. On the contrary, the 9 extra sites that had been identified by Pentara but had passed the SDV were included among the blinded data. This is reasonable. BIVI cautiously attributed overall cognitive improvement in blinded data to a treatment effect, but also hinted their concern; "While patients were randomized 1:1 to NE3107 vs. placebo, a plurality of subjects showed evidence of improvement and may have demonstrated effects unrelated to the administration of the study drug (NE3101 or placebo)". However, before unblinding, the seriousness of the issue could not have been known. The hypothesis at that time was that perhaps the 6 month timeframe was not long enough to wash through all the placebo effect and/or that people just learned to do the assessment because it was repeated 4 times over 6 months. Only after unblinding could it be revealed that cognitive improvement in placebo group at these 9 sites was far beyond what would be expected based on historical placebo data, which led BIVI to exclude and report these extra sites.
There is no evidence that BIVI intentionally misled investors with the blinded data. I commend BIVI for identifying and reporting the misconduct issues. Before blinded data presentation BIVI had conducted SDV on 100% of the documents of all sites. The 6 problematic sites that were identified through this process were excluded from the blinded data presentation. Regarding the rest of the problematic sites (as identified by Pentara), BIVI could not have known the issue before unblinding, as explained in more detail above. Although BIVI was cautiously optimistic about the blinded data, the CEO did warn of potential surprises after unblinding. Personally, as an investor I would have preferred more transparency about the anomallous data observations in some sites that were included in the blinded data. But since the issue could not be assessed before unblinding and these sites had passed the SDV I can't blame BIVI.
As stated by Pentara's CEO the extent of faulty data is unprecedented based on her vast experience in AD trials. Many BIVI investors suspect the trial was sabotaged, but this is not for me to judge here and there is no evidence to support such an allegation at this time.
Phase 3 results from remaining patients
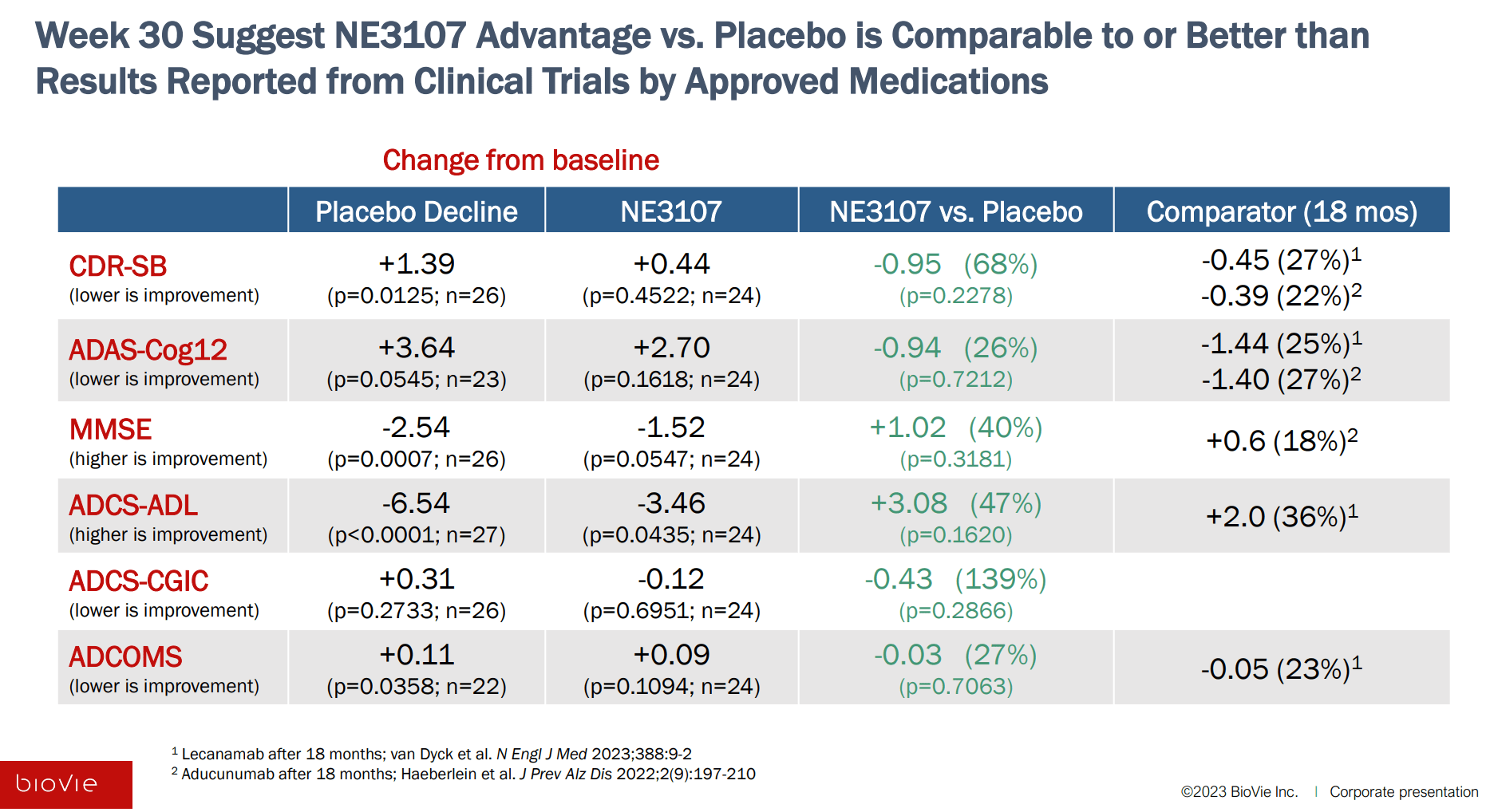
In contrast to expectations based on blinded data, there was no evidence that NE3107 can improve cognition. At the best, NE3107 may delay the rate of deterioration. Nevertheless, even this would be a success considering the safety profile of NE3107 (vs approved anti-amyloid treatments). Notably, consistent benefit over placebo (albeit non-significant) was shown in all measures of cognition, comparing very favorably to approved monoclonal antibodies (which would be a big success for AD patients if proven to be true). Therefore, despite all the limitations there seems to be some promise for AD patients. Adaptive feature of trial will allow BIVI to continue enrolling patients to reach statistical significance. BIVI plans resumption of enrolment within 3-6 months but has not guided yet on the needed sample size to reach statistical significance.
However, I have the following issues with the data;
- Obviously the main issue is the very small number of patients (n=24 in the NE3107 arm and n=33 in placebo arm), resulting in an underpowered study and uncertainty. None of the endpoints reached statistical significance. A larger/longer trial will be needed to confirm benefit.
- There is a big difference in patient numbers between the mITT population (n=81) and the per-protocol population (n=57). The per-protocol population "included those who completed the trial and were verified to take study drug from pharmacokinetic ( PK ) data". However, it is unclear why so many patients are missing, and although asked in the call a clear answer was not given.
- Baseline ADAS-Cog12 in placebo arm was higher vs NE3107 arm (34.4 vs 31.0), indicating worse baseline cognitive impairment.
- Based on the available data BIVI might need a much larger (than the originally estimated) study sample and/or longer follow-up to reach statistical significance, at least for the ADAS-cog12 endpoint. Original estimation about needed sample size was based on assumed difference in ADAS-cog change between NE310 and placebo of -2.5. However, the difference in reported topline was just -0.94, with significantly overlapping confidence intervals and p value of 0.72.
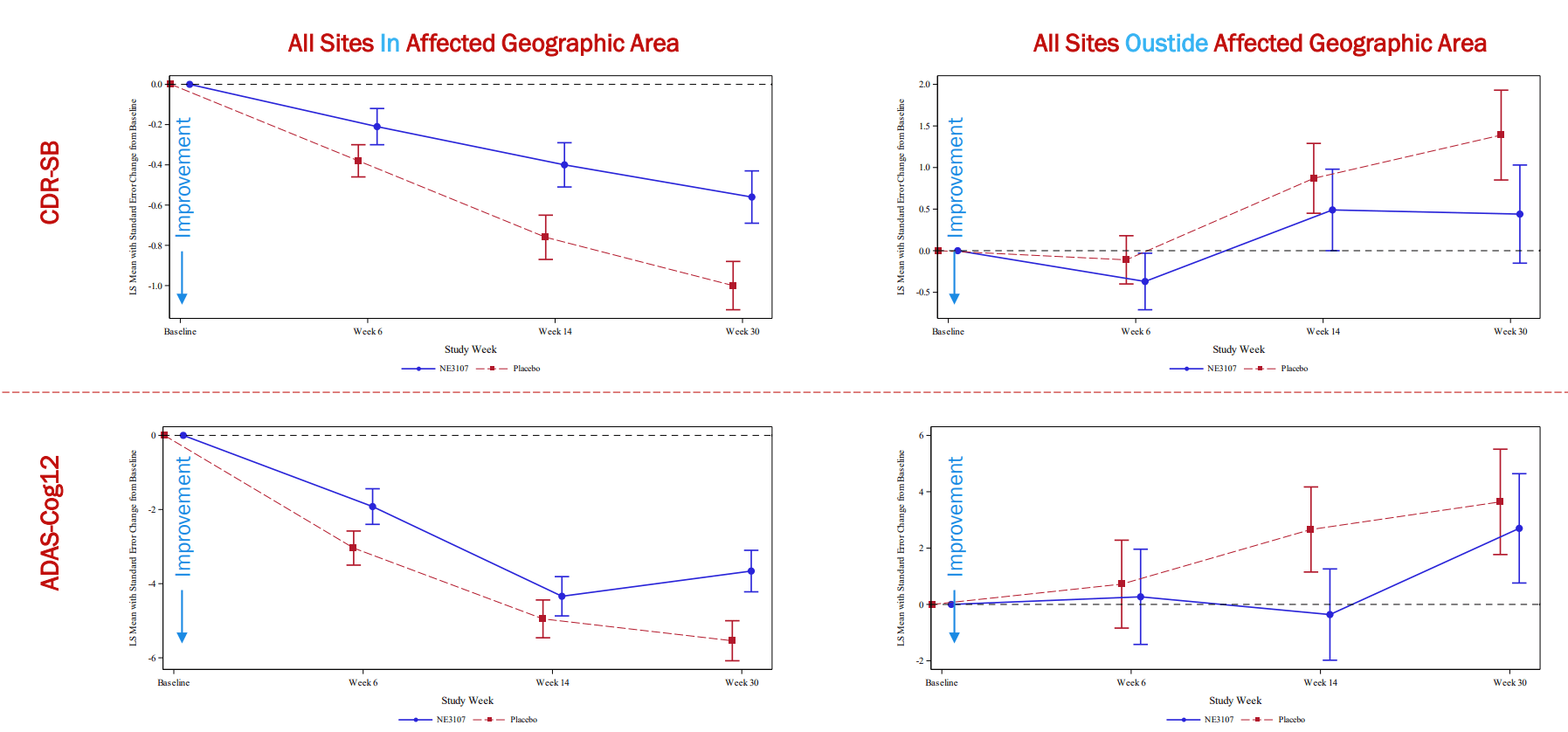
- As shown in the figure below, BIVI has basically excluded all sites in which placebo did better than NE3107 and kept sites in which NE3107 did better. Although there were very valid reasons to do so and the affected sites have been pre-specified before unblinding, this may affect the trust on the very few remaining data.
Comparison of results in affected (n=9 sites) geographic area vs outside affected geographic area. Data on the 6 initially excluded sites were similar to the 9 additional sites identified by Pentara (BIVI presentation) Signals of benefits in cognition (BIVI presentation)
{kind=link}
{kind=link}
What about the biomarker data?
I would consider the following as positive biomarker data; (1) Improvement in biomarkers by NE3107 compared to placebo. (2) Correlation of biomarker improvement with improved cognition. However, to me the presented data can support neither.
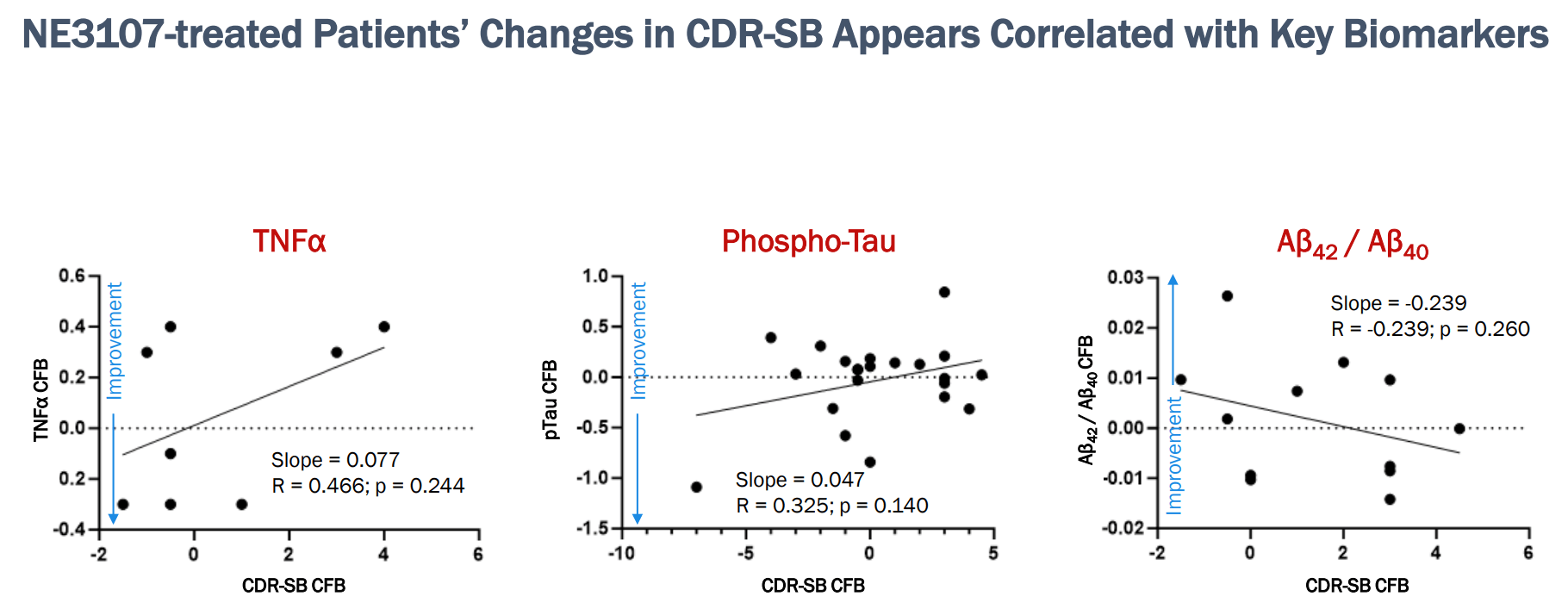
Let's start with the data on TNF, pTau and A?42/??/40;
- Firstly, if you count the data points (e.g. n=8 for TNF) you can see that BIVI does not have all the data yet.
- Then we see no comparison of placebo vs NE3107. So we don't know if biomarkers were improved by NE3107 vs placebo.
- Although there is correlation between these biomarkers and cognition in NE3107-treated patients (which is what you would want to see), without placebo data we can't make any conclusion about treatment effect.
Correlation of CDR-SB with key biomarkers. Note that counting the dots biomarker data appear to be available for only few of the treated patients (BIVI presentation)
{kind=link}
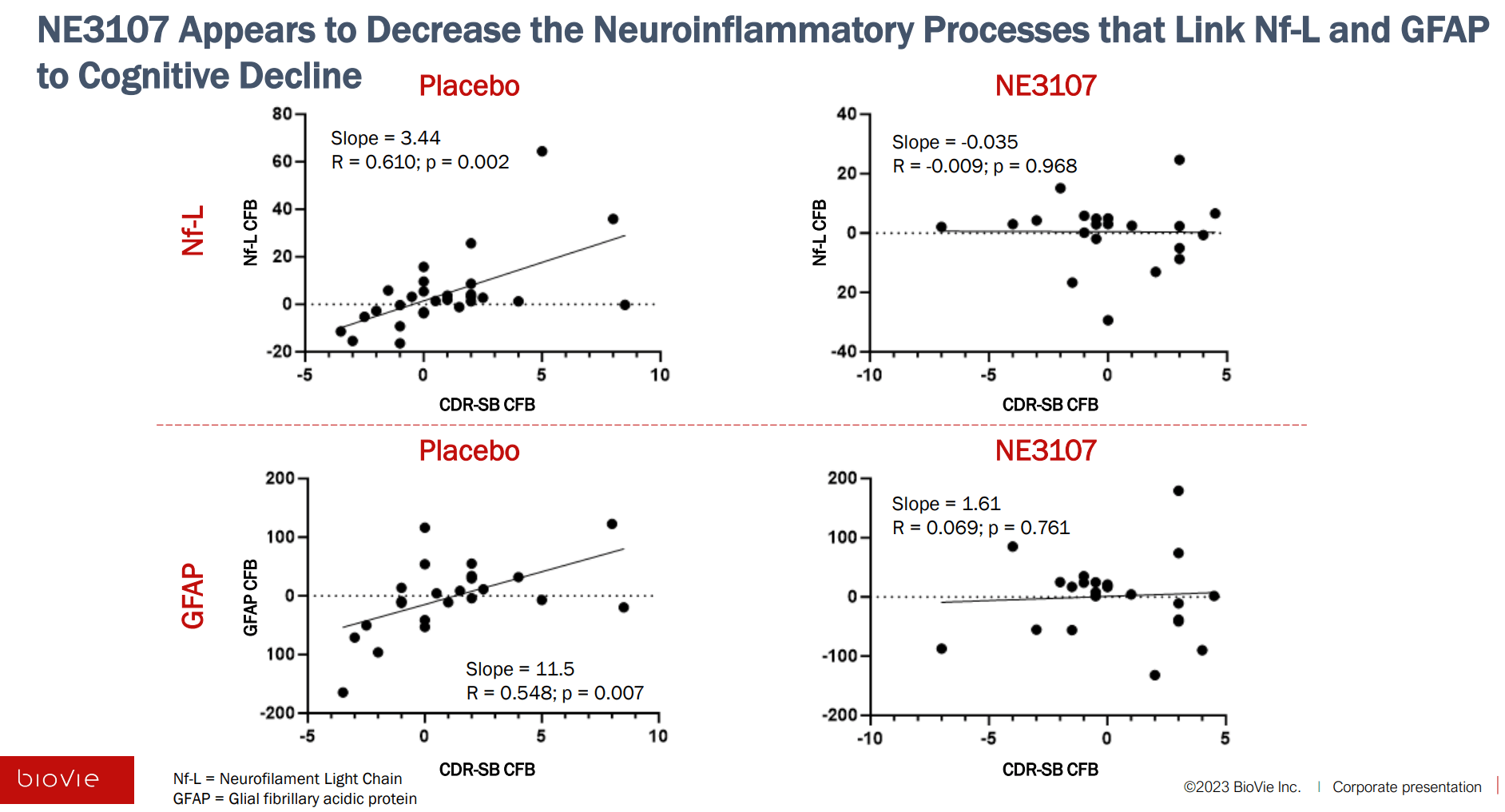
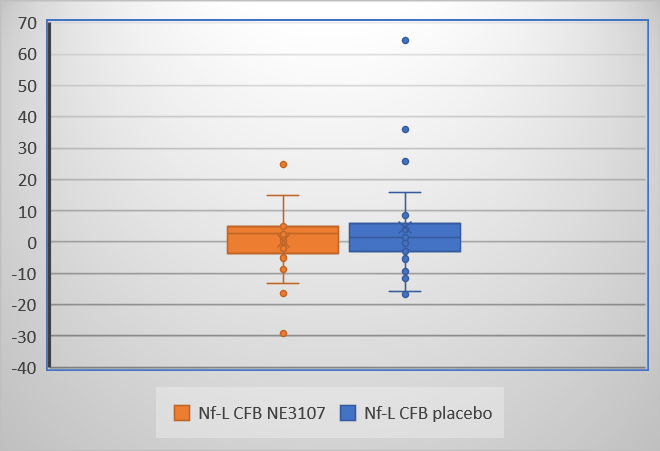
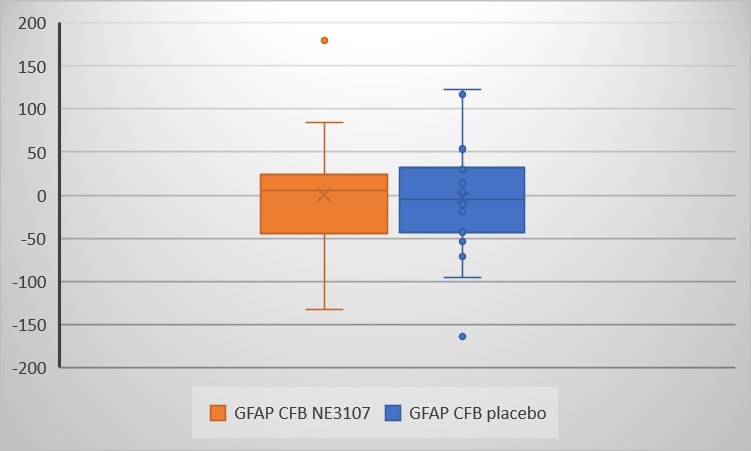
Now let's move on to neuroinflammation biomarker data (Nf-L and GFAP);
- Again no direct comparison of placebo vs NE3107 was provided by BIVI. Nevertheless, I extracted the data (using package "digitize" in R) and I don't see evidence that NE3107 improved biomarkers vs placebo (see figures below).
- The graphs show the expected correlation between biomarkers and cognition in placebo arm. On the contrary, there is no such correlation in NE3107-treated patients (which is unexpected and not what I would want to see). As stated in the title of the slide BIVI's conclusion is that "NE3107 Appears to Decrease the Neuroinflammatory Processes that Link Nf-L and GFAP to Cognitive Decline". As acknowledged by CEO in the call "we don't fully understand this phenomenon yet" and frankly it doesn't make sense to me and cannot consider it a positive finding pending more data on this.
Evidence of reduction of neuroinflammation by NE3107 (BIVI presentation, Slide 10) Boxplot of Nf-L change from baseline (CFB) in NE3107 vs placebo. Data were extracted from above figures using package "digitize" in R (Graph created by me) Boxplot of GFAP change from baseline (CFB) in NE3107 vs placebo. Data were extracted from above figures using package "digitize" in R (Graph created by me)
{kind=link}
{kind=link}
{kind=link}
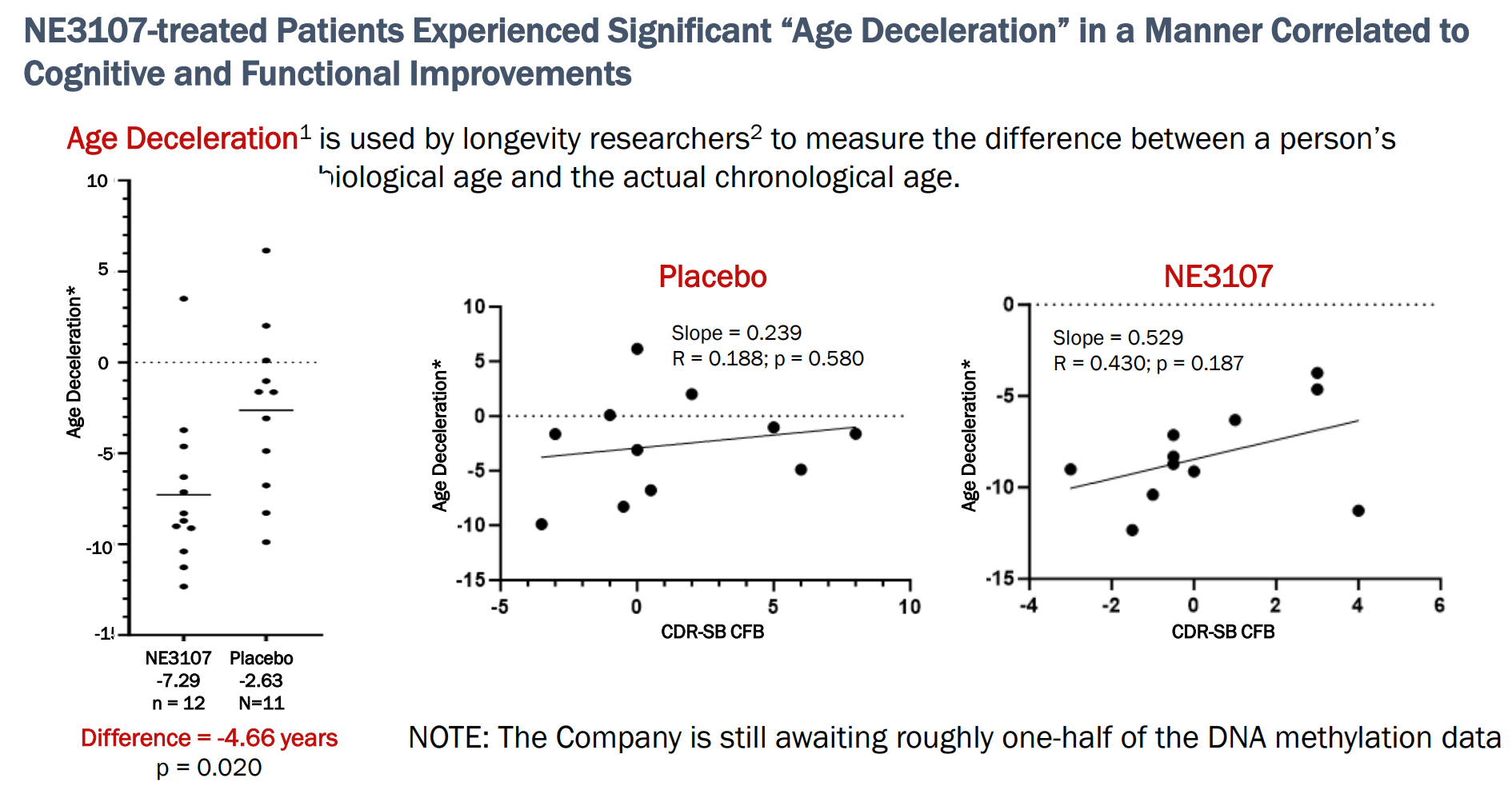
Finally, the epigenetic data;
- Here I finally see what I would want to see; Improvement in DNA methylation comparing NE3107 to placebo AND correlation of such improvement with improved cognition.
- The only (very minor) concern I have with these data is improvement in DNA methylation in placebo as well ("age deceleration" by -2.63 in placebo arm).
DNA methylation data (BIVI presentation)
{kind=link}
To be fair BIVI's team prepared these data on short notice and not all data are available yet. So the full picture may be better than it appears now. Also note again the very small number of patients.
Should we trust these data?
As stated by Pentara's CEO (who has vast experience in AD trials) remaining data are to be trusted because progression in placebo arms matches what is expected based on historical cohorts.
I have the following concerns;
- According to BIVI the CROs' report appears to have identified only 6 sites with serious misconduct issues. The 9 more sites with anomalous data had passed the SDV. Can we be 100% sure that the rest of the sites that had passed the SDV are to be trusted?
- The per-protocol patients were much lower than the mITT patients (discussed above).
- Lack of Nf-L/GFAP correlation with cognition in NE3107-treated patients was an unexpected (for me at least) finding.
What about the rest of the pipeline?
Considering cash balance and setback with the AD phase 3 it is unclear to me what BIVI plans to do with the rest of the pipeline (despite promising early-phase data reported for both Parkinson's Disease and ascites). There are several possible scenarios;
- BIVI might elect to partner/sell any or all of its assets/indications. This might be the best-case scenario for those investing now and for patients. However, partnering assets at this early stage would mean that the value of the deal would be much lower that it would be if BIVI could afford to wait.
- Considering cash balance I wouldn't be surprised if BIVI elected to focus its resources on AD, at least temporarily. BIVI does not have enough cash for not even one phase 3 trial, let alone phase 3 trials for 3 indications.
Financials
BIVI reported cash and cash equivalents of $21M as of September 30, 2023. Total operating expenses were $10.8M (R&D $8.9M, G&A $1.9M). Therefore, BIVI will need to raise cash to keep going, let alone to fund planned phase 3 trials in AD, PD and ascites. R&D expenses during 2023 have ranged from $7M to $11M per quarter, while G&A expenses have ranged from $1.9 to $4.4M per quarter. To support phase 3 trials I am estimating the upper end of these ranges as more representative of what to expect, but this will depend on how many trials BIVI plans to conduct and the timing of initiating these trials. Based on low G&A expenses, and until AD ph3 is resumed, BIVI should have enough cash as there are no ongoing clinical trials to support.
BIVI might be able to get non-dilutive funding from partnerships but whether this can happen soon enough (before dilution is necessary) is unclear. CEO has stated that discussions with potential partners have been ongoing, pending AD phase 3 results. Given the above-discussed limitations of available topline, I am not willing to bet yet on a timely (and/or fair) partnership. Waiting for more clarity on BIVI's financials is a safer approach.
Risks
- As explained above BIVI will need cash to support planned phase 3 trials. At current market cap this can significantly dilute investors, unless BIVI can close a good partnership deal. BIVI would need a good upfront payment to support planned trials. Although all assets are in phase 3 stage, BIVI has moved directly to phase 3 trials after very small early-phase trials. Therefore, I am not sure if potential partners would see BIVI's assets as late-stage assets (which would mean a better deal). Even if BIVI manages to secure a deal, this may not happen soon enough to avoid dilution.
- Another risk is that the setback with the phase 3 trial will significantly delay clinical development of NE3107. BIVI will start re-enrolling the phase 3 but as explained above I expect that a larger sample than originally planned will be need to reach statistical significance. BIVI also may have to conduct another confirmatory trial. This could result in at least 2 years delay (more if a confirmatory trial is necessary) in reaching the market. In the meantime competition may reach commercialization faster.
- There might be legal implications (= legal costs) for BIVI following the phase 3 setback (e.g. already one such lawsuit was announced ). However, this is beyond my expertise to judge.
Conclusions
Investors developed false expectations based on the blinded data presentation. At the time the data were presented BIVI management was aware of misconduct issues in some sites (that did not pass the SDV and were excluded), as well as anomalous data from additional sites (that however had passed the SDV). The seriousness of these issues were much worse than one could anticipate and could be assessed only after unblinding. This, combined with lack of cash and unconvincing topline results, make BIVI a risky investment at least until there is more clarity on its financials. Those with high risk tolerance and/or a long-term perspective may want to buy this dip betting on partnership potential. Personally, I prefer to wait for a few months and re-assess. BIVI remains interesting long-term but the short-term volatility is too unpredictable for me to invest now.
Your feedback is appreciated
Please comment below if you have any feedback (positive or negative), if you spot any mistakes, or if you believe I missed something important in my analysis.
Also I suggest tracking comments if you are interested in following the stock as I may post updates there.
For further details see:
BioVie: Update Following Topline Results (Rating Downgrade)