SAVA - Cassava Sciences: My Bullish Take On Biomarkers And CTAD Data
2023-10-30 03:30:35 ET
Summary
- Cassava Sciences' stock is highly disputed due to conflicting opinions on the science behind its drug candidate, but outside research supports its apparent drug effect.
- Biomarkers show strong reductions in patients treated with simufilam, indicating potential efficacy in Alzheimer's disease.
- The reduction of NfL values over six months is similar to what led to the accelerated approval of Qalsody for ALS.
- Phase 3 trial data, including cognitive maintenance study results, will determine the drug's overall efficacy and potential for approval.
Thesis
The bears and the bulls both have had their way with the stock of Cassava Sciences (SAVA) and probably will continue to do so going forward. The original science surrounding its drug candidate is disputed, though meanwhile outside institutions and new research continue to confirm an apparent drug effect.
The criticism mostly relates to the drug’s mechanism of action, less to human biomarkers and clinical trial results. I try to take a biomarker-based approach looking at many companies in the neurodegenerative and oncology space. To me, Cassava’s biomarkers seem consistent and strong. I fail to see how these could be made up.
The biomarker the scientific community and FDA particularly favor, NfL, has seen strong reductions in simufilam-treated patients. The FDA has granted accelerated approval on the basis of that biomarker in ALS, for the drug Biogen’s ( BIIB ) Qalsody which led to reductions of that biomarker by 55% over 28 weeks compared to a 12% increase in placebo-treated participants. Simufilam appears to do the same in Alzheimer’s patients, over a similar period.
Recent study data from Cassava’s Cognition Maintenance Study confirms the potential of the overall efficacy of simufilam in mild-to-moderate patients, the study population of Cassava’s Phase 3 trials. The data in moderate patients is less inspiring.
A head-to-head comparison with Leqembi or donanemab would be impossible, as both did not target moderate patients, but patients in milder disease stages.
Introduction
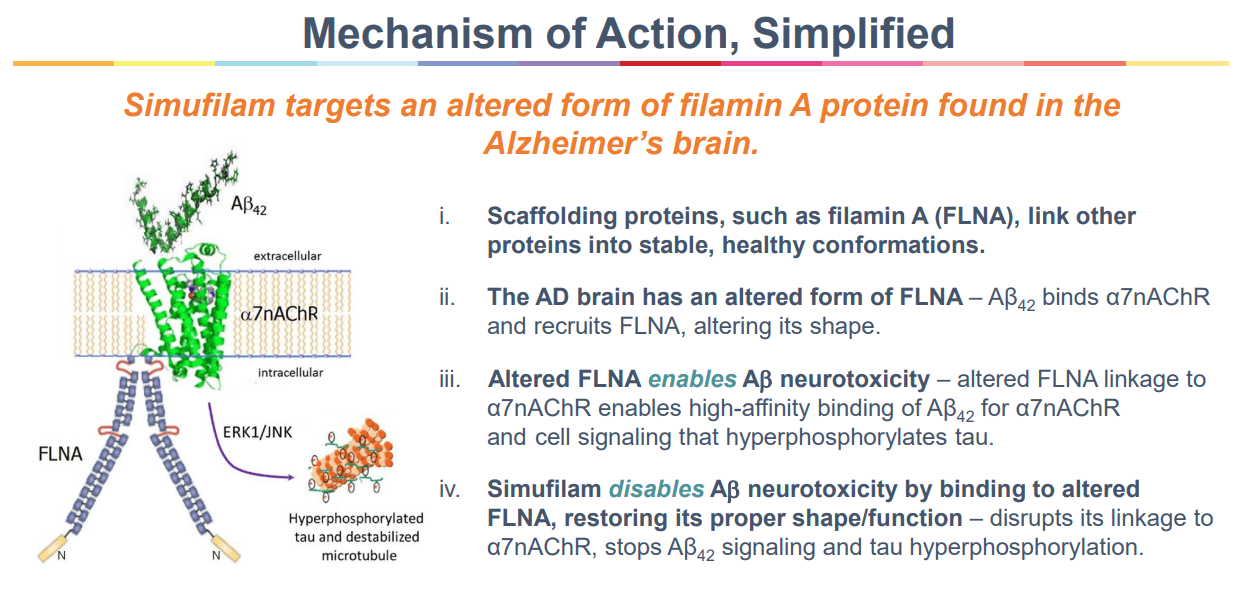
Cassava Sciences is a biotech company with one drug in its pipeline, focused – for the moment – on the treatment of Alzheimer’s disease. Its drug simufilam is said to bind to misfolded filamin A.
As misfolded filamin A allegedly interacts with amyloid-beta and such interaction would lead to inflammatory signaling, a hallmark of Alzheimer’s, simufilam would reverse such inflammatory signaling. Simufilam would restore the normal shape of filamin A. In doing so, simufilam would lead to less neuroinflammation, another hallmark of Alzheimer’s, which would lead to cognitive improvement. I have deliberately included a number of qualifiers in the above explanation to highlight the highly disputed science behind simufilam’s mechanism of action which, I believe, may not yet be fully understood by anyone. Critics of Cassava seem to focus mainly on that scientific part, alleging that the scientific knowledge behind simufilam does not add up and that at least one scientist behind the research work on simufilam did not have the required scientific integrity. This discussion appears to be an eternal back-and-forth. The stakes are also high at this point, with 35% of the available shares shorted , and short presence being systemic since 2021. Either side of the ether here does not grow silent, and I have seen quite some inflammatory comments that have disincentivized me from providing coverage on Cassava Sciences up to this point.
As the current scientific focus and early successes in the field of neurodegenerative diseases focus more and more on the reduction of inflammatory gliosis and biomarkers, and as I have failed to see coverage of what I would consider essential considerations to potential long-term investment or divestments in Cassava Sciences, I wanted to share some of my insights below.
Data will decide
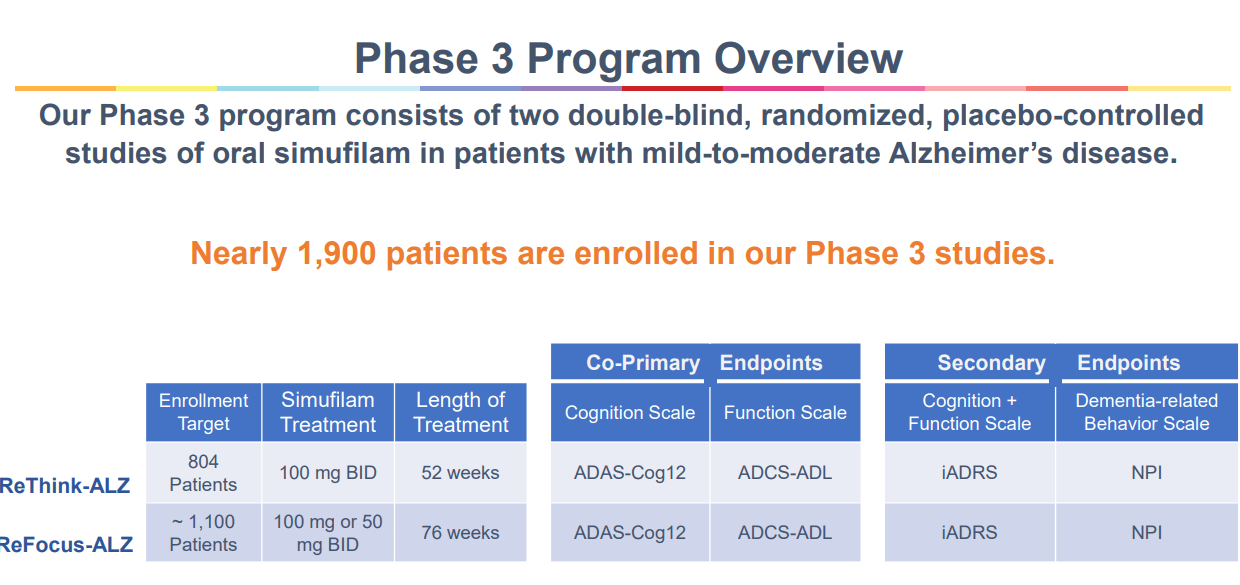
Cassava Sciences should see topline data from its Phase 3 trials in 2025, meaning in a bit more than a year. These trials have enrolled fairly fast, are large, and have a duration of 12 months.
Phase 3 overview (Corporate Presentation)
{kind=link}
If both are successful, then Cassava Sciences has two successful trials and may consider filing for approval in Alzheimer’s disease.
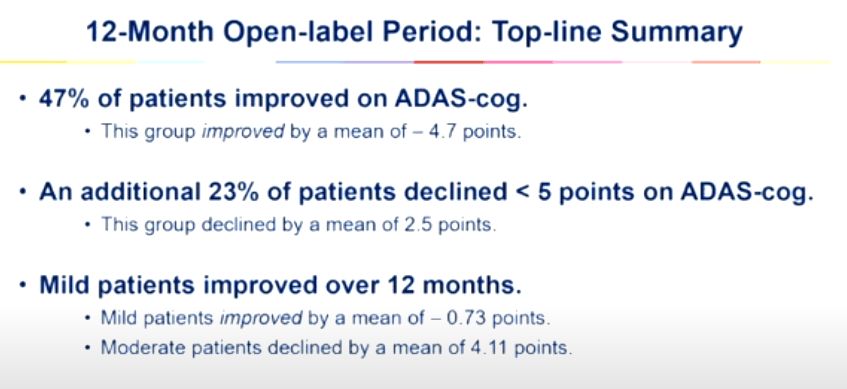
These are the results from the twelve-month open label study.
Summary open label study (Cassava Sciences CTAD presentation)
{kind=link}
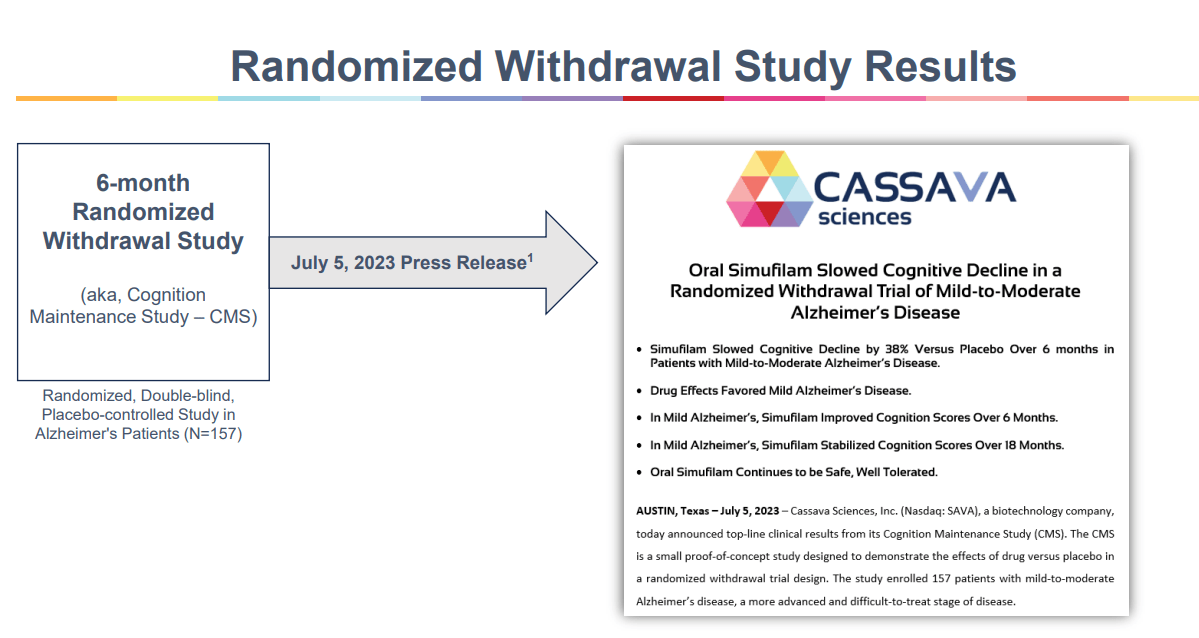
The results of the Cognition Maintenance Study, which was a six-month randomized placebo-controlled trial after patients had been twelve months on simufilam already, hence generating data of use versus placebo after an initial twelve months on the drug, can then serve as additional proof of long-term efficacy.
CMS study results (Corporate Presentation)
{kind=link}
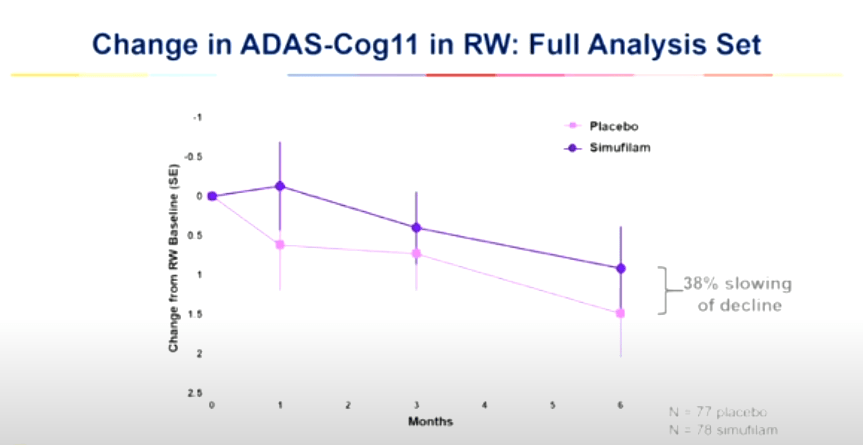
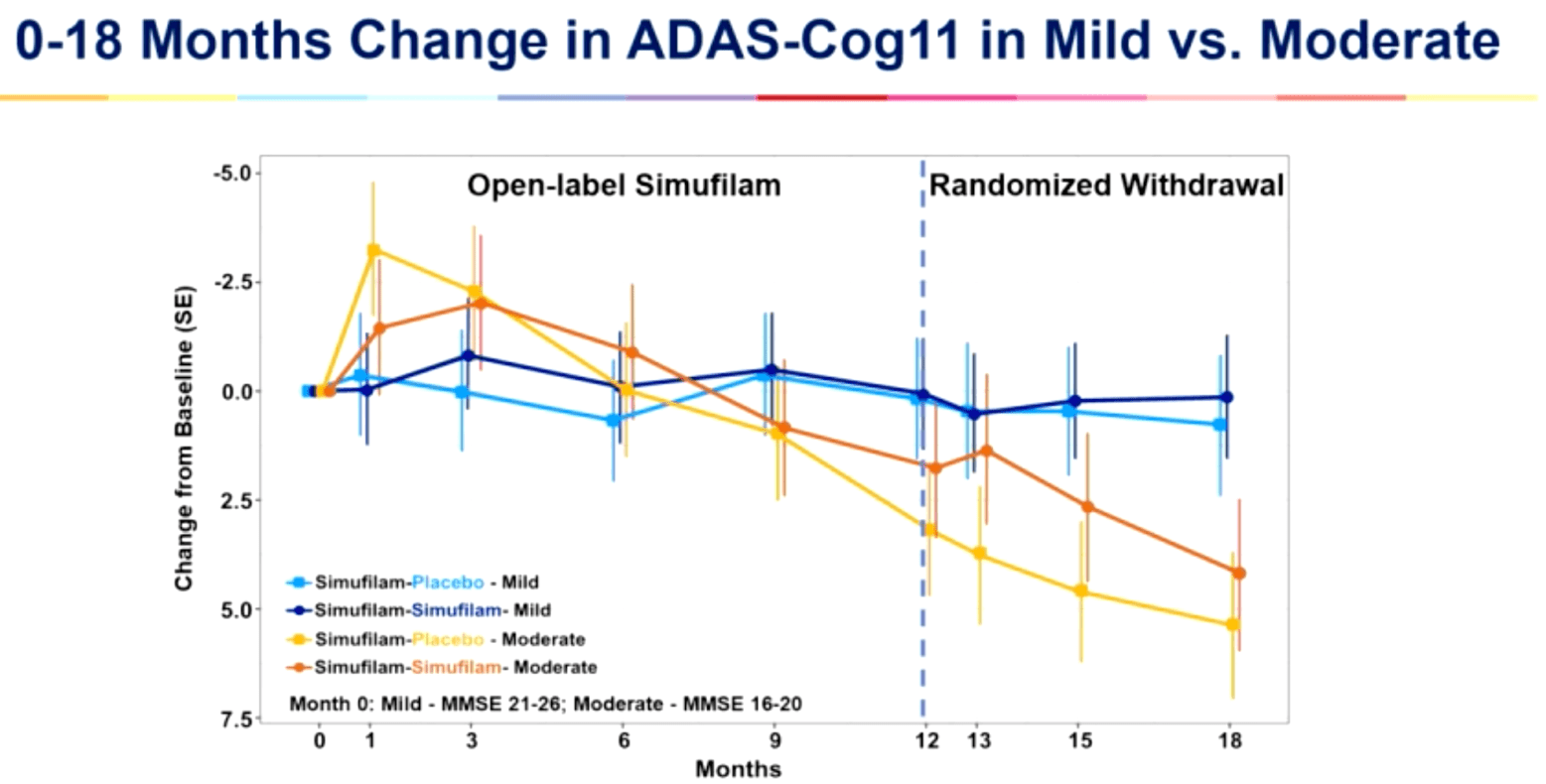
A similar effect is seen in the Cognition Maintenance Study, where simufilam slowed cognitive decline by 38% versus placebo, with efficacy in mild patients being stronger.
Adas-Cog11 change CMS study (CTAD 2023 presentation)
{kind=link}
Total change 18 months (CTAD 2023 presentation)
{kind=link}
Though at this time the data is either non-placebo-controlled or not statistically significant, it could outperform Biogen’s Leqembi and Eli Lilly’s ( LLY ) donanemab if reproduced in the Phase 3 trials. Two arguments may play in favor of better results. Patients in the CMS study had already been on drug for a year, which could mean maximum efficacy had already been reached. Apparently , at the time of enrolling in the CMS study, some patients who had been at the moderate end of disease in the open label study had further declined to the severe stage, which may explain the further rapid progression of these patients. I do note, however, that the above result appears far from what had initially excited the market in February 2021.
Two ongoing Phase 3 trials are ongoing, and both have become the object of a Citizen Petition requesting they be suspended. The FDA dismissed that request as it was one-sided and as it did not pass the formal test as to whether the particular request could be made in a Citizen Petition. Since that time, three camps seem to have arisen; the investors, the non-investors, and those that have decided it is better to refrain from investing. Though it had already been denied, the request for trial suspension recently saw new daylight, in light of the alleged discovery and coverage of a draft report of CUNY as to whether one of the scientists having researched the mechanism of action of simufilam is responsible for any wrongdoing. Cassava considered that the CUNY report made no findings of data manipulation and referred to a new short attack. CUNY has meanwhile distanced itself from the report. I think chances are small, the FDA actually believes that it ‘should’ do anything at this stage. It is, however, not excluded that we see a new Citizen Petition from new short-sellers, on the basis of new facts, which again may not be able to tackle the afore-mentioned formal hurdle, but may provoke a further-declining share price. For the record, Cassava Sciences is fighting a legal battle against some short-sellers.
If the FDA would however halt trials at this stage, with a drug proven to be safe, remarkable open-label and placebo-controlled results, testimonials, biomarkers, and strong support from Cassava shareholders, I believe it would do something utterly against the very idea of clinical trials, which are designed to see whether patients benefit from the drug. If they do not, the somewhat 1,900 patients in Phase 3 trials of simufilam may sadly join the already abundant number of patients that have ever been in the abundant failed trials for Alzheimer’s, e.g., anti-amyloid antibodies or BACE inhibitors. That is, alas, the reality of any clinical trial; many fail, some succeed, and patients are at a loss when they fail. Last year, an article appeared questioning the very science on which these anti-amyloid antibodies are based. Nonetheless, I have not seen a Citizen Petition or other similar request, requesting that such trials, though proven to be unsafe, be halted.
Moreover, anti-amyloid antibodies are known to be unsafe, contrary to simufilam. An unsafe therapy should be a red flag, which many physicians and several Advisory Committee members have voiced when Aduhelm was about to receive accelerated approval on the basis of reduction of amyloid beta as a surrogate endpoint.
The biomarkers
Introduction
As Alzheimer’s is a human disease, it would make sense that clinical data in humans is what the FDA will look at most in the end. Though one can only guess at this stage what Cassava’s Phase 3 trials will report, one can meanwhile have a look at the biomarkers that have already been reported by Cassava Sciences.
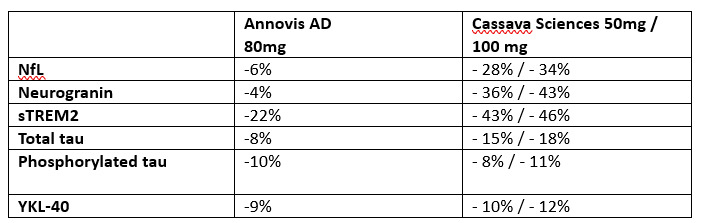
That is what I look at mostly throughout my work, and which is the basis for my strong conviction in INmune Bio. In my coverage of Annovis, which I am more skeptical about, I had made a comparison with data on different biomarkers reported by both companies. I copied some here.
Comparable biomarkers Annovis - Cassava Sciences (28 days) (Own Work)
{kind=link}
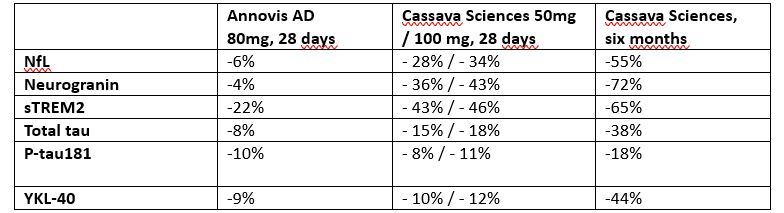
What is striking here is the consistency of data coming from Cassava Sciences’ simufilam. On average, Cassava’s results appear about 3-4 times as strong as those of Annovis, and what’s more, Cassava’s biomarkers massively improved at the six-month time point. If we include those, we get the following.
Comparable biomarkers Annovis - Cassava Sciences (Own Work)
{kind=link}
For the record, these are not all biomarkers reported by Cassava Sciences, but those that I considered fit for comparison with another drug candidate and which were available for all time points.
Biomarkers of neuroinflammation/glial activity
YKL-40 is a well-established biomarker of neuroinflammation. In Alzheimer’s disease, its expression is often seen in astrocytes, the brain’s most abundant immune cells or glial cells, more particularly in clusters around amyloid plaques. The inflammatory gliosis mentioned above refers to a chronic state of moderate inflammation produced by these glial cells, including microglia. The idea behind anti-inflammatory treatments for Alzheimer’s is that by reducing their inflammatory phenotype, they may be able to revert to their original function, which is taking care of the brain, a function that they have given up by remaining in an inflammatory state for too long.
Another marker of the reactive and pro-inflammatory state of glial cells is sTREM2, a marker particularly of microgliosis. Microglia are less abundant than astrocytes but have been identified as equally important in the architectural processes of the brain.
The reduction by simufilam of both YKL-40 and sTREM2 by 44% and 65%, respectively over the course of six months, indicates to me that a very strong anti-inflammatory response is being generated by simufilam. I would not understand how these biomarkers could be indicative of placebo-like efficacy, rather to the contrary, they prove that simufilam has an effect on a cellular level.
In that respect, as TREM2 is an important genetic risk factor for Alzheimer’s disease, Alector ( ALEC ) has a monoclonal antibody in trials targeting TREM2 on microglia in Alzheimer’s and AbbVie has been given an option to develop and commercialize AL002, for milestones potentially totaling $487.5 million.
But sTREM2 and YKL-40 are no markers of neurodegeneration.
Biomarkers of neurodegeneration
Total tau and p-tau181 could be seen such as neurofibrillary tangles of tau protein demonstrating loss of structure in tiny vessels inside the neurons. Neurogranin is also a marker of neurodegeneration, but not one that is as established as NfL.
That brings me to NfL. NfL is a biomarker that should be able to have value across neurodegenerative diseases, both as a measure of the speed of neurodegeneration as well as a measure of regeneration, treatment effect in other words. In MS , ALS , and AD , the scientific community appears to align on its prognostic value, also in AD in Down syndrome, Creutzfeldt-Jakob’s disease, and FTLD . Increased NfL levels in AD have been associated with neuronal death and axonal degeneration. Its correlation with cognitive decline has been established more than once also outside of Alzheimer’s disease. This is striking as one would consider hallmarks of disease, e.g. amyloid aggregates and neurofibrillary tau tangles, as most predictive of disease evolution or treatment effect. That is, however, not the case.
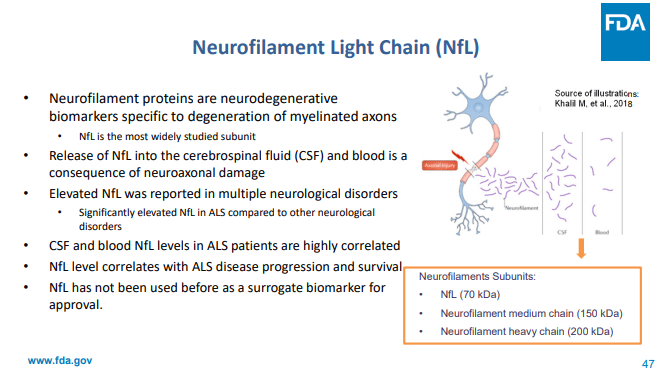
NfL, to me, is by far the most important biomarker reported by Cassava Sciences, as it has given way to accelerated approval of Biogen’s tofersen/Qalsody [ FDA slideshow , meeting transcript , briefing document , approval PR ].
NfL slide briefing FDA for tofersen/Qalsody approval (FDA)
{kind=link}
Tofersen’s trial results did not reach the trial’s primary endpoint, however, treatment with Tofersen showed a 55% decrease in NfL values over 28 weeks, all while patients on placebo saw an increase of 12%. The accelerated approval was preceded by a unanimous vote by the Advisory Committee considering that, in spite of the trial’s failure, as a surrogate endpoint plasma NfL could reasonably likely predict clinical benefit in SOD1-ALS. Considerations of the Advisory Committee had been, among others, the FDA’s own detailed analysis including available literature and data providing enough evidence to support NfL as a surrogate endpoint, and the idea that delaying approval for an indication with such high unmet need may be unethical.
Tofersen reduced NfL values in ALS by 55% over 28 weeks. Simufilam does exactly the same over a similar period of time, a 55% decrease over six months. I am seeing some potential caveats. The indication is not identical, with NfL levels being particularly elevated in ALS. There is a possibility that these biomarker results originate from patients in milder stages of disease, as it had appeared that the initial results posted by Cassava Sciences had come mostly from patients at milder stages of AD. These data are generated from a small and more particularly open label study and hence may not lead to accelerated approval as such, but it is hard to imagine the values of 25 patients would be erroneous or manipulated. If patients on placebo would have a 55% decrease in that biomarker, Cassava’s data are strong, but they are not the best ever reported, which could validate them. Apart from similar numbers from Tofersen in ALS, INmune Bio’s ( INMB ) Xpro showed an 84% reduction of this biomarker over the course of three months in AD patients. For further reference, Alector’s AL001, targeting the progranulin gene for frontotemporal dementia, saw a 27% reduction over the course of 7 months. Biogen’s Leqembi saw reduction of biomarkers of inflammation but did not see reduction of NfL. Data on Eli Lilly’s donanemab should still be published, I believe. In a failed trial, Roche’s (OTCQX:RHHBF, OTCQX:RHHBY, OTCPK:RHHVF) gantenerumab slowed NfL’s worsening, with treated patients seeing that biomarker go up 1.7% compared to 3.4% for placebo. These are larger trials and it says something about the normal evolution of NfL as a biomarker.
BioVie ( BIVI ) should report NfL data in January 2023, after its topline Phase 3 readout in about a month’s time. For Anavex (AVXL), more than a year after my coverage in which I had mentioned that I would wait for biomarker data to consider my final position on the company, I am still awaiting the entire biomarker readout which should include NfL data.
Full approval / accelerated approval
Cassava Sciences is currently on a path towards traditional full approval for Alzheimer’s disease.
As it now appears that simufilam may perform better in patients with mild AD and less good – or not - in patients with moderate AD, I consider it possible but not certain whether those trials will succeed in reaching statistical significance. My take is that Cassava’s chances of success are higher than those of failure, but the moderate group may pull down the overall result. If Cassava Sciences had known this in advance, perhaps the better choice would have been to start trials in MCI and mild AD, just like big pharma most often does it, as these patients seem more likely to have a treatment effect. I again repeat another point I have made before on many other companies, and that is – for Cassava Sciences - that the levels of misfolded filamin A in the AD population are not yet well enough established in literature, and that therefore it is not excluded that patients without such sufficiently elevated levels may not sufficiently benefit from simufilam.
Cassava’s recent presentation at CTAD showed that some patients who were considered moderate were actually already at the severe stages of disease, which may play in favor of Cassava’s Phase 3 trials. However, Cassava will have lots of biomarker data from that Phase 3 trial, which should include NfL data. If so, in case Cassava e.g. sees strong efficacy in mild patients which appears likely, the company may try to go for accelerated approval on the basis of the exceptionally strong biomarker data, particularly NfL. A confirmatory trial may in such case need to be run, e.g. in mild patients alone, if already both Phase 3 trials wouldn’t be able to sufficiently make that distinction by themselves.
The above does not cover all potential ways toward approval. I am aware supporters of Cassava Sciences have been in favor of Cassava Sciences being granted Breakthrough Therapy Designation.
Outside confirmation of simufilam’s effect
It now appears that four academic institutions have generated data in support of the biological activity of simufilam. This includes a Parisian lab confirming that simufilam potently reduced amyloid ? binding to ?7nAChR, with a different technique than had been used before. That seems to align with simufilam’s proposed MoA as shown below:
Simufilam MoA (Corporate Presentation)
{kind=link}
The latter research also includes this phrase:
Simufilam at 100 fM, 10 pM or 1 nM reduced the release of inflammatory cytokines tumor necrosis factor ? (TNF?), interleukin ((IL))-6 and IL-1? by approximately 75% or more (p < 0.001; Figure 3).
For me, this sentence, even if it comes from preclinical work, is a strong validator of simufilam’s potential efficacy. As noted in earlier coverage of different companies in the space by myself and in two and potentially more articles by Seeking Alpha analyst Vision and Value under the common title ‘Capitalizing On Inflammation's Role In Neurological Disease’, tackling inflammation while allowing for homeostasis may be essential to treating neurodegenerative diseases. Both BioVie ((BIVI)) and INmune Bio ((INMB)) have correlated reduction of TNF with cognitive efficacy, and this builds on several meta-analyses showing that non-selective and non-brain-penetrant TNF inhibitors lead to reduced risk of Alzheimer’s disease. A reduction of the above cytokines by 75% is not nothing, but I do note one caveat; entire TNF signaling should not be inhibited to allow for homeostasis; one will want the microglia and astrocytes to perform their nurturing and brain-architectural functions. INmune Bio’s Xpro selectively targets soluble TNF. I have not seen research on simufilam’s capabilities in this respect, but I am willing to think they may be generated one day, seeing a seemingly lasting effect at least in milder patients.
Outside validation is a strong element playing in favor of simufilam’s efficacy. In light of this, though some have considered it to be useless to confirm safety of a drug that has placebo-like efficacy - it seems legitimate to me that Cassava confirms that simufilam is safe.
Some critics have compared Cassava Sciences to Theranos, but insofar as I know, Theranos’ claims were never validated by outside parties. To properly dispute simufilam’s effects, I believe one would have to invalidate these outside validations. Insofar as I am aware, no outside paper has been retracted or has been under scrutiny. I am therefore inclined, again, to consider simufilam as a potential therapy for Alzheimer’s disease.
Finances
As of June 30, 2023, Cassava Sciences had $168.4 million in cash and cash equivalents. Cassava Sciences has a cash burn rate of about $66 million per year, which should allow it to finalize its Phase 3 trials and finance further research.
Risks
On both sides of the positioning of Cassava Sciences, I have seen strong-minded investors. That may become a risk when every person with a potential counterargument may become classified as pro or against.
I have quoted trial design risks and risks related to the lack of strong scientific background on filamin A’s involvement in Alzheimer’s disease, and if so, to what extent and in how many patients.
Further short involvement and allegations are possible, as Cassava Sciences is the object of constant debate among investors.
Finally, at any time, risks and potential benefits of an investment need to be open for reassessment, particularly as developments in the pharmaceutical industry can change rapidly. In the coming year, such developments could among others come from BioVie ((BIVI)), Annovis (ANVS), Alzheon [private], and Athira Pharma (ATHA).
My position
At this time, I have not taken an investment in Cassava Sciences, mostly because of the unpredictability of whatever next action will be taken by either side. In the current case of Cassava Sciences, my biomarker-based approach has little predictive value for the stock’s moves, so I prefer to invest in potentially overlooked stocks with similar potential.
The afore-mentioned considerations do imply my bullishness on simufilam’s potential, and save for further unexpected events which may alter my ideas, I plan to take an investment in the stock prior to the Phase 3 readout if at that time the market cap would still be such that significant upside is possible in case of success. That is, however, a long time out, and with the statistical chances of 2024 turning out to be bearish being low, I will have to see how things play out.
It is for the above reasons that I give Cassava Sciences a Bullish rating, more for the potential of its drug candidate than for the unpredictability of its stock movements.
Conclusion
For a long time at this point, my bullishness on simufilam as a drug candidate for Alzheimer’s disease has been based on biomarker data, mostly because of the 55% reduction of NfL values over the course of six months. The other biomarkers reported by Cassava Sciences appear to align with this reporting, which could explain why Cassava Sciences has reported good cognitive data in patients with mild Alzheimer’s disease. Further outside confirmations of simufilam’s efficacy, including a Parisian lab that also saw massive reductions in major pro-inflammatory cytokines, confirm that stance.
The stock’s volatility and unpredictable short actions are a concern, and a fair analysis needed to include caveats, for example with regard to the Phase 3 trials which include moderate patients and the unknown percentage of Alzheimer’s patients who have sufficiently elevated levels of misfolded filamin A to respond to treatment.
If simufilam, shown to be safe, could reproduce similar results as those seen before, this time in Phase 3 trials and with statistical significance, then I would be in favor of it having its place on the market one day. If an efficacy signal would only be detected in mild patients, then the NfL data could allow for an accelerated approach plus confirmatory study similar to how Biogen’s Qalsody was approved.
For the reasons mentioned above, I give Cassava Sciences a bullish rating.
For further details see:
Cassava Sciences: My Bullish Take On Biomarkers And CTAD Data