BMYMP - Geron: Ready To Face The Competition With Imetelstat In Lower Risk Myelodysplastic Syndromes
2023-05-31 09:47:21 ET
Summary
- Geron Corporation's imetelstat has shown a clear benefit in treating lower-risk myelodysplastic syndromes (LR-MDS), with positive results in its phase 3 IMerge study.
- Imetelstat is likely to receive FDA approval for LR-MDS, with a potential priority review and a possible launch in H1 2024.
- Geron faces competition from Bristol-Myers Squibb's Reblozyl, but imetelstat's efficacy in heavily transfusion-dependent patients may provide differentiation from its competitors.
Geron Corporation ( GERN ) is developing imetelstat for lower risk myelodysplastic syndromes (LR-MDS) and myelofibrosis ((MF)). While GERN announced success in its phase 3 IMerge study in LR-MDS in January 2023, the MF indication isn't as close to approval with an interim analysis not expected from a major phase 3 study until 2024. As such, this article takes a look at GERN's odds of approval in LR-MDS and the competition, current and potential, in that indication.
Figure 1: GERN pipeline. Note that the IMerge study has already produced a positive readout. (GERN website.)
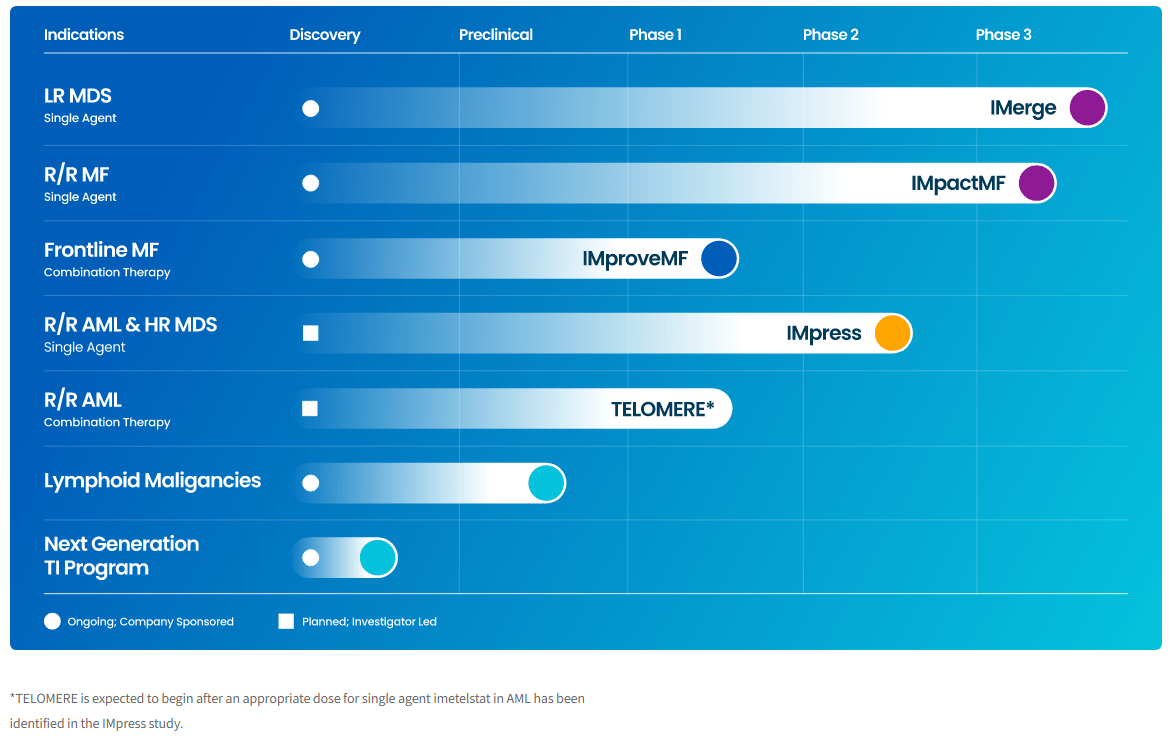{kind=link}
Imetelstat: Ready for regulatory submission in LR-MDS
GERN's IMerge study recruited patients with LR-MDS who were either refractory to, or ineligible for, erythropoiesis stimulating agents (ESA). If you can't take a drug to stimulate erythropoiesis you might be needing a lot of blood transfusions. GERN's imetelstat, a telomerase inhibitor, has the ability to reduce the need for blood transfusions in LR-MDS.
On January 4, 2023, GERN announced that its IMerge study met the primary endpoint with 39.8% of imetelstat treated patients achieving transfusion independence of 8 eight weeks or more, compared to just 15% of patients in the placebo group (P < 0.001). Splitting the data into patients with a type of cell in their blood called ringed sideroblasts (RS+), and those without ringed sideroblasts (RS-), we see that imetelstat outperformed placebo in both groups. Another way of splitting the data is to look at patients with very high transfusion burden, who require more than six transfusions every eight weeks, compared to those with high transfusion burden, again we see that imetelstat outperformed placebo.
Figure 2: Screenshot of the table of results from GERN's IMerge study of Imetelstat in LR MDS. (GERN press release, January 4, 2023.)
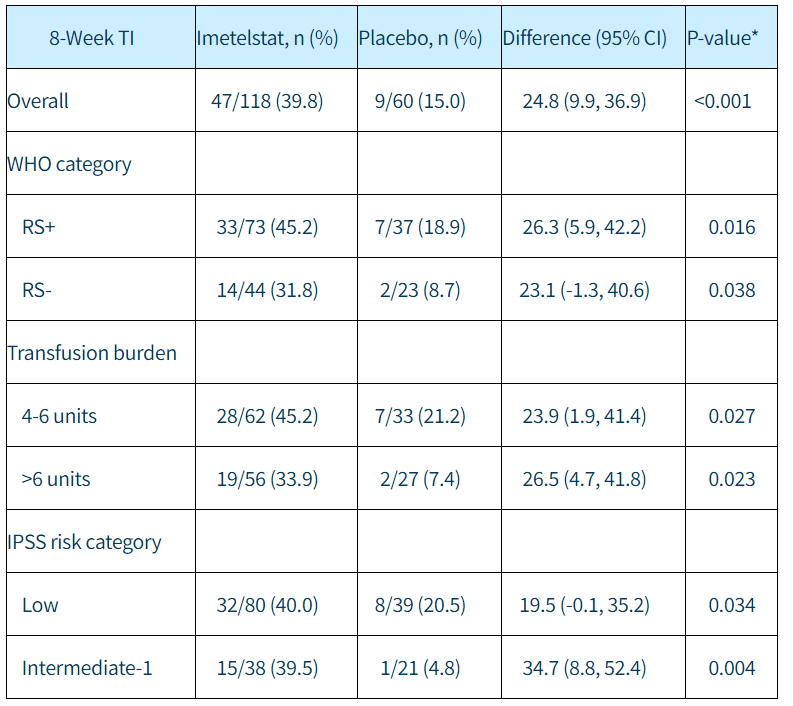{kind=link}
On the safety side, while there were reductions in various cell counts, such as low neutrophil count (neutropenia), they were manageable and so the rate of serious infections wasn't significantly increased by imetelstat. Similarly, while there were increases in serum levels of certain liver enzymes, there were no Hy's law cases, which means we would predict imetelstat to go on to cause drug-induced liver injury.
GERN sees a total addressable market of ~ $3.5B in LR-MDS, where the IMerge study has already shown a clear benefit of imetelstat, and ~ $3.5B in myelofibrosis, for which imetelstat has the IMpactMF study. With regards to the IMpactMF study , we won't see anything until a 2024 interim analysis. Nonetheless, results from a phase 1 combination study of imetelstat with ruxolitinib in MF (IMproveMF) could come by year-end 2023, so the MF indication is still worth considering even in the near-term.
An existing competitor: Reblozyl
At this point it is worth mentioning a major competitor in LR-MDS, Bristol-Myers Squibb's ( BMY ) Reblozyl (luspatercept), which is already approved in patients with RS+ very low- to intermediate-risk MDS who require at least two units of red blood cells every eight weeks.
Figure 3: Screenshot of Prescribing Information for luspatercept, note the LR MDS indication. The beta thalassemia indication isn't relevant to this discussion. (Reblozyl Prescribing Information from Reblozyl website.)
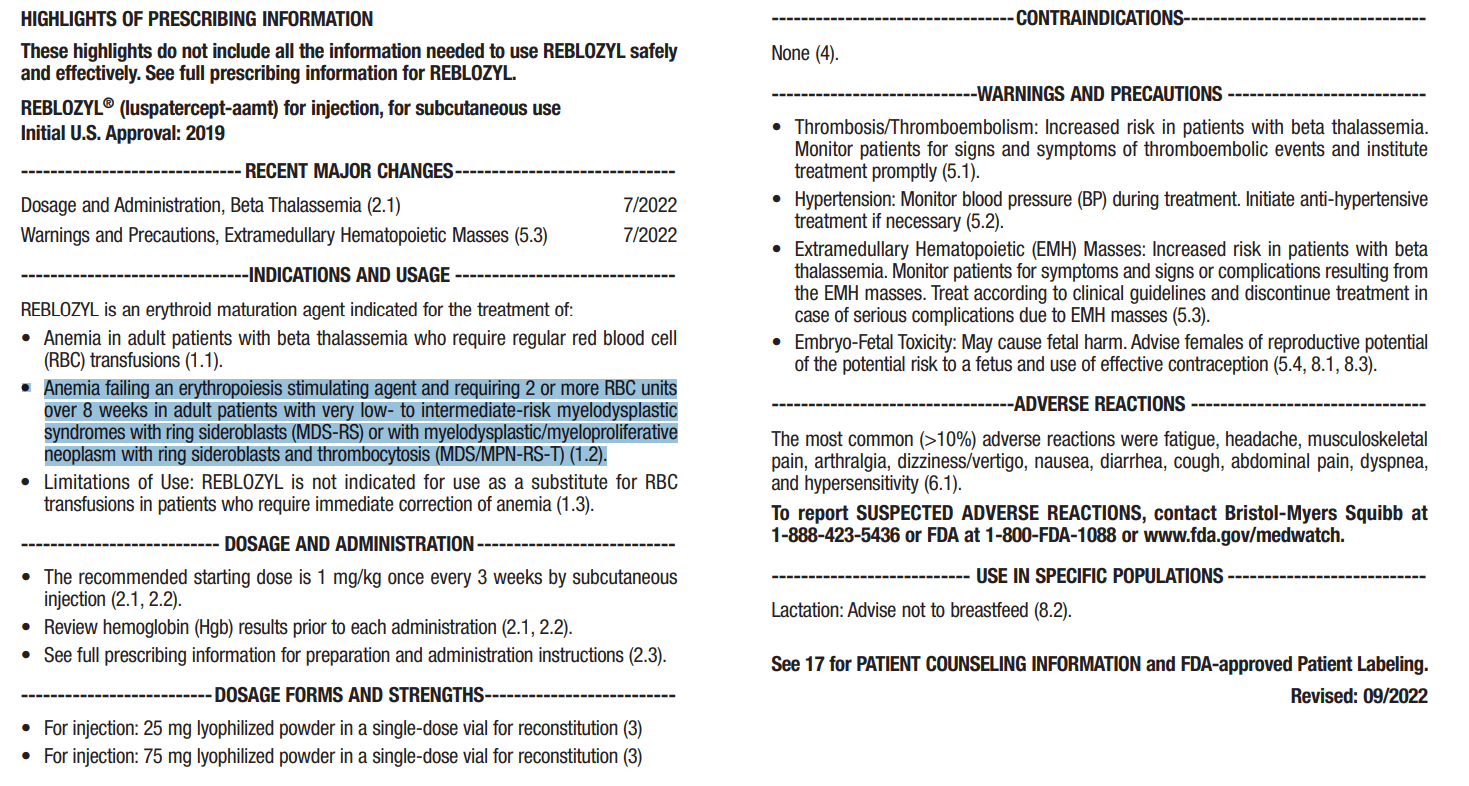{kind=link}
The approval of Reblozyl in the MDS indication was supported by the double-blind, placebo-controlled, phase 3 Medalist study in very low- to intermediate-risk MDS patients. In the Medalist study , 38% of patients treated with luspatercept achieved transfusion independence of at least eight weeks during weeks 1-24 of the study. By comparison, just 13% of the placebo group achieved the eight week transfusion independence endpoint.
Figure 4: Percentage of patients achieving transfusion independence in the phase 3 Medalist study of luspatercept (Reblozyl) in MDS. (N Engl J Med 2020; 382:140-151. )
Comparing the results of GERN's IMerge study to the Medalist study of Reblozyl, Evaluate Vantage's Jacob Plieth notes that while Medalist didn't provide data from RS- MDS patients, it still sees off-label use in RS- patients, and so the real differentiator for imetelstat might be the data in patients with high transfusion burden. In Medalist, in the subgroup of patients requiring at least six units of red blood cells per eight weeks at baseline, just 9% (6/66) of patients treated with imetelstat achieved transfusion independence for eight weeks or longer. This was still more than the subset of placebo group patients with very high transfusion burden, where just 1% (1/33) achieved transfusion independence of at least eight weeks. Recall that in Figure 2 above, imetelstat produced a 33.9% rate of eight weeks or more transfusion independence, in patients requiring more than six units of red blood cells per eight weeks at baseline.
While Medalist looked at patients who had failed an ESA, were unlikely to respond to an ESA or had discontinued an ESA due to an adverse event, there is data for Reblozyl outside of that patient group.
Reblozyl in ESA-naive patients
On October 31, 2022, BMY announced positive topline results from a phase 3 study of Reblozyl vs epoetin alfa (an ESA) in ESA-naive patients with very low/low/intermediate-risk MDS. Actual percentages on transfusion independence weren't presented at the time of the press release, but we can learn a little more about this trial from the most recent abstract discussing it, available on May 25, 2023, as part of the 2023 annual meeting at the American Society of Clinical Oncology ((ASCO)).
The ASCO abstract notes that 58.5% of patients treated with luspatercept achieved the primary endpoint of red blood cell transfusion independence (RBC-TI) of ? 12 weeks, with a concurrent mean hemoglobin increase of ? 1.5 g/dL within the first 24 weeks. By comparison 31.2% of patients treated with epoetin alfa achieved the primary endpoint. Put simply, luspatercept performed nearly twice as well as an ESA in initially ESA-naive patients (essentially a first-line setting).
As such, while the previous LR-MDS treatment paradigm might have been simpler (Figure 5), with patients failing first-line ESA's progressing to Reblozyl or imetelstat (if approved), the treatment paradigm may have changed somewhat as of late 2022.
Figure 5: GERN overview of the LR MDS treatment landscape. Note the existence of data from trials of luspatercept as a first-line agent may change the treatment landscape. (GERN Corporate Presentation, May 2023.)
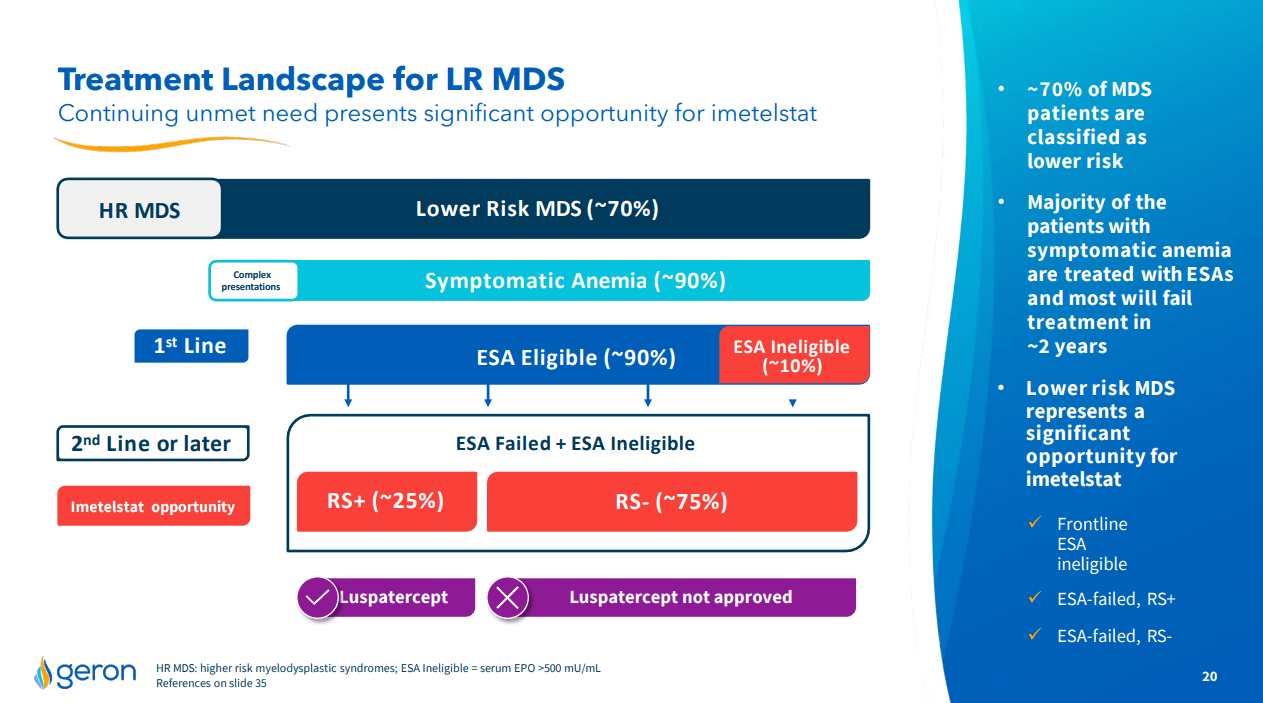{kind=link}
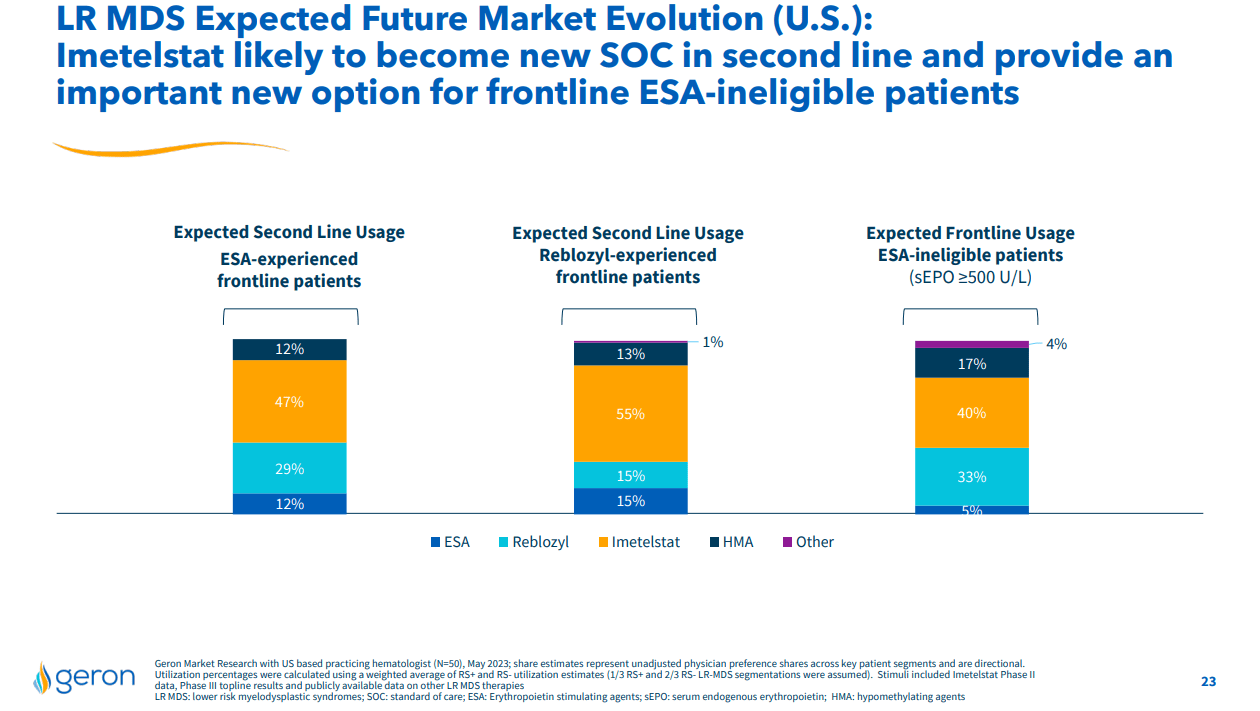
Still, even if patients had to try Reblozyl first, imetelstat can still see use, and GERN is aware of this possibility. For example, GERN's May Corporate Presentation includes a slide noting that based on a market research with 50 US practicing hematologists, there is an expected 55% utilization of imetelstat in "Reblozyl-experienced frontline patients," (Figure 6, middle column).
Figure 6: Results from market research in 50 US hematologists. (GERN Corporate Presentation, May 2023.)
{kind=link}
Odds of FDA approval for Imetelstat in LR-MDS
I think it is likely the FDA will approve GERN's imetelstat in LR-MDS, especially based on the strength of the efficacy data in heavily transfusion-dependent patients. Further, while Reblozyl might see off-label use in RS- MDS patients, GERN's IMerge study provides double-blind, placebo-controlled data in RS- patients who are refractory or ineligible for ESA's.
With regards to the safety of the drug, I don't think there is anything so concerning as to prevent approval. I think the safety can be considered by the prescriber in the context of that efficacy and the severity of a given patient's condition. Even though we don't have much data from luspatercept refractory patients, physician experience in this scenario can grow over time and of course GERN could agree to run studies in that population as part of a post-approval requirement.
I really don't see the safety issues or the fact that the treatment landscape has changed with luspatercept as being likely to result in imetelstat being rejected by the FDA. Instead I'd consider that there is always a chance of an New Drug Application (NDA) not being approved because of a chemistry manufacturing and controls ((CMC)) issues. GERN has never got a drug approved and so while they may have an experienced team, the outfit itself hasn't proven itself in that regard.
GERN is set to submit its NDA in June with a pre-NDA meeting already completed and leading to no change in submission plans, that bodes well for the odds of approval. GERN has requested a priority review, which would see a review time of six months, following an initial two month period for the FDA to file or refuse-to-file the NDA. An eight month review period overall then would allow approval in Q1'24 and the H1'24 imetelstat launch GERN is preparing for.
Financial Review
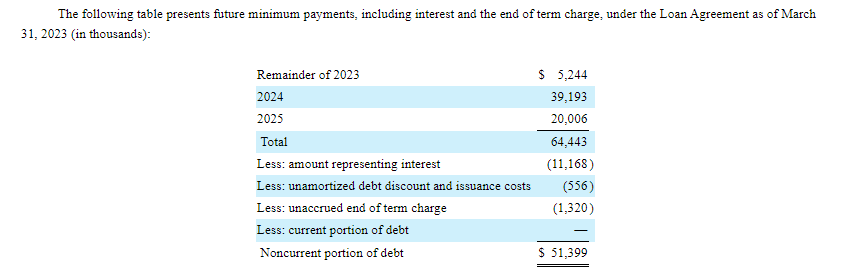
GERN reported Q1'23 earnings on May 11, 2023. The company had $409.2M in cash and marketable securities as of March 31, 2023. R&D expenses were $27.2M in Q1'23 and G&A was $12.9M. Net loss for Q1'23 was $38.1M and net cash used in operating activities was $46.4M. GERN predicts its current resources will fund operations until the end of Q3'25 and we're somewhat dependent on that prediction as the current rate of cash burn wouldn't be a good estimate of cash burn going forward as the company moves from the late clinical stage to the commercial stage. It should be noted that GERN has $51.4M in noncurrent debt from its loan agreement set up in 2020 with Hercules and Silicon Valley Bank.
Figure: Screenshot of payments to be made under the current terms of GERN's loan agreement. (GERN 10-Q, filed May 2023.)
{kind=link}
In any case, GERN's cash and marketable securities balance, net of its debt, of $350M+ means GERN doesn't need to find a partner to launch imetelstat in LR-MDS.
As of May 5, there were 508,766,846 shares of GERN's common stock outstanding, corresponding to a market cap of $1.67B (at $3.28 per share).
Conclusions
GERN is executing in the clinic with success in IMerge, and other studies set to readout in late 2023 (phase 1), 2024 (IMpactMF interim) and beyond. I think the drug is likely to get a priority review given the options available to patients failing an ESA or Reblozyl are limited and the drug offers a compelling benefit in LR-MDS patients with high transfusion dependence. On the commercial side GERN is well prepared having got a cash raise out of the way in Q1'23 meaning further dilution is unlikely in the near-term.
I view GERN as a buy based on a number of catalysts ahead of which I expect most to break in the company's favor. The first would be the acceptance of the imetelstat NDA for substantive review (likely in August, two months after June submission) rather than a refusal-to-file letter. The second would be the potential for the FDA to grant a priority review, rather than a standard review, and the third would be the possibility of positive results from a phase 1 combination study of imetelstat and ruxolitinib in MF in late 2023.
The risks of any long in GERN are several fold, a few of which are worth discussing here. Firstly, any delays in submitting the imetelstat NDA in June could cause the stock to fall. Secondly, a CMC issue is always a possibility leading to refusal-to-file letter, which would cause GERN stock to fall, as would a refusal-to-file letter for any other reason. Lastly, GERN's imetelstat NDA might not be granted a priority review, which could also cause the stock to fall.
For further details see:
Geron: Ready To Face The Competition With Imetelstat In Lower Risk Myelodysplastic Syndromes