MOR - MorphoSys: A Buying Opportunity Following Mixed Phase 3 Results In Myelofibrosis
2023-11-27 14:00:44 ET
Summary
- MorphoSys announced positive topline results from its phase 3 trial of pelabresib in frontline myelofibrosis, nearly doubling spleen volume reduction (the primary endpoint) compared to placebo.
- However, key secondary endpoints assessing symptomatic improvement did not reach statistical significance in the total population. Nevertherless, significant improvement was shown in the pre-specified intermediate-risk subgroup (majority of enrolled patients).
- Totality of the evidence supports the approval of pelabresib, which could have a significant multi-billion dollar market potential. MorphoSys plans regulatory submissions in the US and Europe in mid 2024.
- Considering a projected cash runway into 2025, regulatory delays could have a significant negative impact. Beyond pelabresib, no other major catalyst is expected within the projected cash runway.
Thesis overview
MorphoSys AG ( MOR ) recently announced positive topline results from its phase 3 trial of pelabresib in myelofibrosis (MF). The study easily met the primary endpoint. However, despite the strong positive trend, statistical significance was not achieved at key secondary endpoints assessing symptomatic improvement. Nevertheless, in a pre-specified subgroup analysis in intermediate-risk patients (majority of enrolled patients), statistically significant symptomatic improvement was demonstrated. Overall, the totality of the evidence supports approval in my opinion. MOR plans regulatory submissions in the US and Europe in mid 2024. A detailed presentation of the topline results is expected at ASH 2023.
The focus of this article is pelabresib's potential in myelofibrosis. Success of pelabresib is a major determinant for further growth of MOR. I will not discuss in detail here the sales and label-expansion potential of Monjuvi (MOR's approved product) or the rest of the pipeline.
Brief overview of myelofibrosis
Myelofibrosis refers to a myeloproliferative neoplasm characterized by bone marrow fibrosis, cytopenias (low blood cell counts), constitutional symptoms, hepatosplenomegaly, and/or extramedullary hematopoiesis. Patients are at risk for premature death from disease progression, leukemic transformation, thrombohemorrhagic complications, and infections. Pathogenesis of myelofibrosis is partly associated with constitutive activation of the JAK/STAT pathway (hence the development of JAK inhibitors for treatment of MF), resulting in clonally expanded megakaryocytes cluster in the bone marrow, infiltration by neutrophils, inflammation and ultimately bone marrow fibrosis (resulting in cytopenias and extramedullary hemopoiesis, the latter being the cause of splenomegaly).
Allogeneic hematopoietic cell transplantation is currently the only curative option, but patients are often not eligible either due to comorbidities or advanced age. Pharmacological treatment with a JAK inhibitor ((JAKi)) is recommended only for symptomatic high-risk patients not eligible for HCT, with splenomegaly, anemia and platelet counts above 50000/?l.
Targeting disease modification in myelofibrosis
Currently approved pharmacological treatments aim for symptom control and/or reduction of transfusion dependency, rather than disease modification, but do not appear to have significant disease modifying potential. Disease modification in myelofibrosis would mean improved overall survival and/or normalization of hematopoiesis and improvement in bone marrow fibrosis. Targeting just the JAK/STAT signaling appears to be an insufficient approach, with major limitations ;
- On-target anemia and thrombocytopenia. Treatment-emergent myelosuppression is particularly limiting as many patients have disease-related cytopenias. These JAKi cannot be used in patients with a platelet count of less than 50000/?L and should be used with caution in patients with severe or transfusion-dependent anemia.
- JAKi do not prevent leukemic progression, which is a key contributor to mortality in MF.
- Patients eventually become intolerant, refractory, and progress after treatment with JAKi.
- While some novel JAKi, such as momelotinib and pacritinib, may allow patients with disease-related anemia and thrombocytopenia to enjoy the benefits of this therapy, there is likely a limit to targeting this pathway.
To overcome the limitations highlighted above, novel targets are being explored outside the JAK-STAT pathway, either as monotherapy or as add-on therapy to JAKi.
Natural history of myelofibrosis and potential time points for intervention. Earlier intervention is more likely to achieve disease modification. Hence the study of pelabresib-ruxolitinib combination in JAKi-naive patients. (Cancer . 2022 Jul 1;128(13):2420-2432.)
Background on pelabresib
Pelabresib is a BET inhibitor aimed to be used in combination with JAKi for myelofibrosis. MOR acquired pelabresib from Constellation Pharma at $1.7B. The acquisition was not perceived well by investors for several reasons; (1) High cost of the acquisition, (2) To fund the acquisition MOR sold royalty rights (mostly of Tremfya) to Royalty Pharma, (3) Once a discovery powerhouse, MOR had to resolve to buying the pipeline from another biotech, (4) Not only that, but MOR also halted preclinical R&D development and out-licensed the rest of Constellation Pharma's oncology pipeline, in order to reserve cash for its late-stage pipeline.
Overview of topline phase 3 results
MANIFEST-2 was a phase 3 randomized, placebo-controlled trial evaluating pelabresib (vs placebo) in combination with ruxolitinib (a JAKi) for JAKi-naive myelofibrosis patients. MANIFEST-2 followed very promising results in a previously uncontrolled phase 2 study (MANIFEST) which showed that the combination in JAKi-naive patients was significantly better compared to what would be expected from historical monotherapy JAKi data.
The primary endpoint in MANIFEST-2 was the proportion of patients achieving at least a 35% reduction in spleen volume (SVR35). The rationale for this endpoint is that it is a strong predictive marker for survival (in other words, patient that achieve higher spleen volume reduction are expected to survive longer). Key secondary endpoints (the rationale for these will be explained in the next section) were; TSS50 (proportion of patients showing at least 50% improvement in the Total Symptom Score) and absolute TSS change. The latter was added in the protocol after a MOR meeting with the FDA in September 2023. As explained by MOR, it is a reasonable addition. TSS is a continuous variable and absolute TSS change helps better quantify the symptomatic, if any, benefit of adding pelabresib. Other meaningful endpoints include the following; duration of splenic and symptom response, hemoglobin response (?1.5 g/dL from baseline), bone marrow fibrosis (BMF), progression-free and overall survival.
To sum up the results (which were presented by MOR in a webinar);
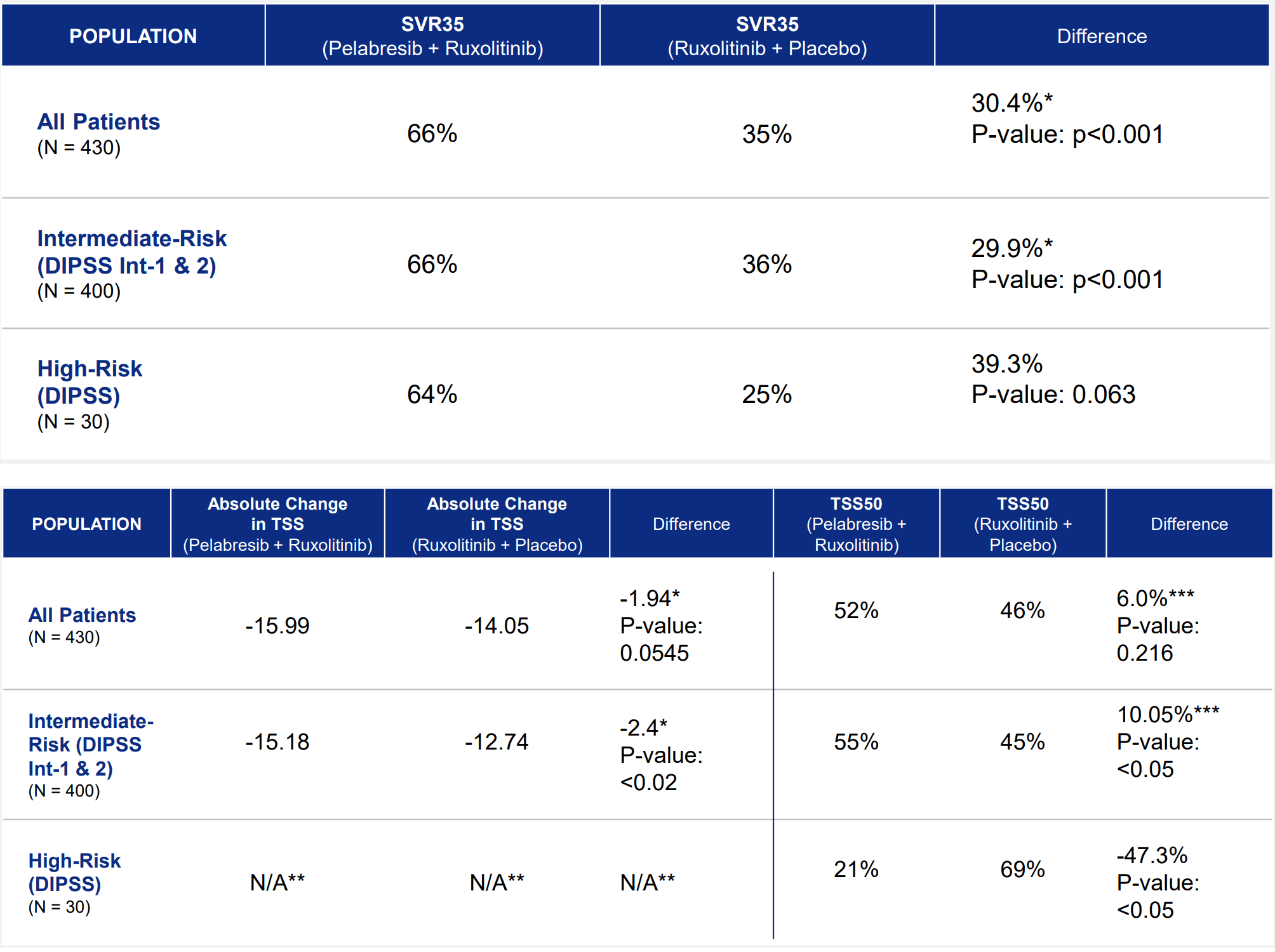
- MANIFEST-2 met primary endpoint, nearly doubling SVR35 response rate (66% versus 35%)
- The key secondary endpoints assessing symptom reduction, TSS50 and absolute change in TSS, showed significant improvements for intermediate-risk patients (p<0.05, p<0.02, respectively) and strong numerical improvements for overall population
- The MANIFEST-2 results show a greater proportion of patients achieved hemoglobin response (? 1.5 g/dL from baseline)with the pelabresib and ruxolitinib combination than with placebo and ruxolitinib. Details on this endpoint were not presented.
- Pelabresib and Ruxolitinib Combination Was Well-Tolerated. Details on this endpoint were not presented.
A more detailed presentation is planned for ASH, December 10. Data on BMF from MANIFEST-2 have not been reported yet. However, reduction of BMF has been shown in MANIFEST. Furthermore, endpoints on progression-free and overall survival are awaited from longer-term follow-up of MANIFEST and MANIFEST-2. Results on these endpoints are of major importance for the commercial success of pelabresib.
{kind=link}
Results in primary and key secondary endpoints of MANIFEST-2 (MANIFEST-2 Results - Conference call )
So why is the stock price down?
As explained in a Fierce Biotech article , "The MorphoSys CEO has previously said AbbVie “failed” its phase 3 myelofibrosis trial because the Big Pharma missed one of two endpoints. Now, Kress is defending MorphoSys’ similarly mixed data". Specifically, rival navitocalx has met the primary endpoint (SVR35) but failed to meet the TSS50 endpoint.
But why are TSS endpoints so important considering impressive benefit in the primary endpoint? Spleen volume reduction alone as an outcome is not meaningful for patients and clinicians unless associated with other supportive findings, such as meaningful symptomatic improvement, less need for transfusions and/or better survival. Therefore, it is reasonable that SVR alone may not support approval. Hence the role of the key secondary endpoints. I couldn't find ABVV's phase 3 data on TSS50 endpoint for comparison. However, pelabresib's results are not that bad, showing positive trend in the total population and statistically significant symptomatic improvement in the intermediate-risk subgroup. Although investors don't like biotechs resorting to the "totality of the evidence" argument to support approval, in the case of pelabresib, I do believe that the totality of the evidence does support approval.
Evidence of disease modification
The rationale for pelabresib-ruxolitinib combination is to overcome above-discussed limitations of JAKi-monotherapy, including eventual non-response to treatment and/or eventual disease progression. Fortunately, there is promising evidence of disease-modifying potential from the pelabresib-ruxolitinib combination from the ongoing MANIFEST phase 2 study;
- At least one grade improvement of BMF in 27% of evaluable patients at 24 weeks, which was maintained in 59% of those at or beyond the next assessment
- Declustering in bone marrow megakaryocytes
- Reduction of Janus Kinase 2 allele (V617F), a biomarker that indicates a potential biological response in myelofibrosis. A reduction of at least 20% was shown in 38% of evaluable patients.
Long-term outcomes (progression-free and overall survival) are awaited from both MANIFEST and MANIFEST-2.
Totality of the evidence
To sum up the above, MANIFEST 2 has shown that
- Pelabresib impressively improved SVR35 (a major predictive marker of survival), the primary endpoint, nearly doubling SVR35 compared to placebo. The benefit was consistent in both high- and intermediate-risk patients.
- Pelabresib significantly improved TSS50 and absolute TSS change in the pre-specified intermediate-risk subgroup, which represents the majority of enrolled patients. However, absolute benefit in TSS50 and TSS change was small. Furthermore, the key secondary endpoints did not reach statistical significance in the total population, and, surprisingly, pelabresib did significantly worse than placebo in high-risk (n=30) patients. Hopefully, there will be some more clarity on that in the upcoming ASH oral presentation.
- Pelabresib showed a greater proportion of patients achieved hemoglobin response (? 1.5 g/dL from baseline). This is important, because worsening anemia is a major toxicity of ruxolitinib therapy.
In addition, findings from the ongoing MANIFEST study suggest disease-modifying potential, a major limitation of currently approved treatments.
Competition
As can be seen in the figure below, and discussed in more detail in recent publications ( 1 , 2 , 3 ), there are several drugs under development with disease-modifying potential. However, in Clinicaltrials.gov I could find only two ongoing phase 3 studies of novel agents (non-JAK/STAT-targeted) in JAKi-naive MF patients (=target population of pelabresib);
- Selinexor + ruxolitinib ph1/3 ( KPTI ); Top-line data from the ph3 are expected in 2025 . Results of the phase 1 part were impressive ; "At week 24, 91.7% (11/12) of efficacy evaluable patients demonstrated SVR35 and 77.8% (7/9) achieved TSS50. The intent to treat population achieved a 78.6% (11/14) SVR35 and 58.3% (7/12) TSS50 respectively". "As of the August 1, 2023 data cut-off date, all patients treated with 60mg selinexor and who achieved ?35% reduction in spleen volume (SVR35) at week 24 (n=11), continued to remain in radiographic response. In addition, all of the seven patients who achieved TSS50 at Week 24 remained in response as of the data cut-off". This compares favorably to pelabresib and navitoclax (below), but the study was very small (n=12). KPTI will have an oral presentation at ASH, December 10 entitled "Selinexor Plus Ruxolitinib in JAK Inhibitor (JAKi)-Naïve Patients with Myelofibrosis: Long Term Follow up from XPORT-MF-034 Suggestive of Disease Modification".
- Navitoclax + ruxolitinib ph3 ( ABBV ); The study met the primary endpoint (SVR35 at w24) but did not meet the first ranked secondary endpoint of improvement in patients’ TSS from baseline to week 24 (similar to MANIFEST-2). I could not locate specific TSS results in ABBV's ph3. In the preceding phase 2 study (REFINE, NCT03222609, Cohort 3), treatment with navitoclax in combination with ruxolitinib resulted in SVR35 and TSS50 in 52% and 31% of the patients at week 24, respectively (vs 66% and 52%, respectively, in MANIFEST-2). Reduction in bone marrow fibrosis has been shown, similar to pelabresib in MANIFEST (35% of the patients had ? 1 grade reduction "at any time post-baseline" vs 28% at 24w in MANIFEST). "The company plans to wait for additional follow up data on the primary, secondary and other endpoints, expected in the fourth quarter of this year, before engaging with regulatory agencies regarding potential next steps." Based on above data, pelabresib seems to have the advantage (at least based on SVR35 and TSS endpoints), however, which one of the two treatments has better disease-modifying potential remains unclear to me.
The list above does not include;
- Ongoing earlier-stage (ph1/2) studies.
- Studies in the 2nd-line setting, i.e. relapsed/refractory-JAKi patients (not the target population of pelabresib). Notable examples; bomedemstat ( MRK ), navtemdalin (Kartos Therapeutics), imetelstat ( GERN ), tagraxofusp (Stemline). But the list is much longer.
- Studies of novel (e.g. jaktinib) or approved (e.g. pacritinib, momelotinib, fedratinib) agents targeting the JAK/STAT signaling. "While some novel JAKi, such as momelotinib and pacritinib, may allow patients with disease-related anemia and thrombocytopenia to enjoy the benefits of this therapy, there is likely a limit to targeting this pathway", as explained in a section above.
- Studies of agents targeting symptom-control or anemia, rather than aiming for disease modification (e.g. pomalidomide , luspatercept ).
- Parsaclisib, which has been discontinued .
A detailed discussion of treatments under development is beyond the scope of this article. From an investor's perspective, there doesn't seem to be much ph3-stage competition in the 1st-line, JAKi-naive setting. Such competition may emerge in the future from earlier stage (ph1/2) programs, or expansion to 1st-line of agents currently under development as 2nd-line options. Furthermore, pelabresib will have to prove disease-modifying activity in the long-term. How good pelabresib's disease-modifying potential is remains to be proven, although evidence so far (discussed above) is promising.
Novel and potentially disease-modifying therapeutic targets in myelofibrosis (Cancer . 2022 Jul 1;128(13):2420-2432.)
Market potential
MorphoSys estimates that there are about 18,000 intermediate-/high-risk cases in the US that are eligible for systemic treatment. Incyte, which markets ruxolitinib, estimates that about half (which would correspond to 9,000) of these eligible patients receive ruxolitinib. Approval of pelabresib would mean that all these patients would become eligible to receive the combination, rather than ruxolitinib monotherapy. Recently approved momelotinib has a list price of $26,900 for a bottle of 30 tablets, corresponding to $323K/year/patient. At a similar price, the market potential for pelabresib (assuming 9,000 patients) is $2.9B just in the US. MorphoSys has bet a lot on this and needs this win.
Potential of pelabresib expansion to other myeloid indications
Beyond myelofibrosis, which is now the priority, pelabresib has promising potential for other myeloid disorders as well. Notably, in Arm 4 of MANIFEST a 60% complete/partial hematologic response has been demonstrated plus symptomatic improvement (50% TSS50 and 31% median reduction in TSS) in patients with high-risk essential thrombocythemia resistant/intolerant to hydroxyurea. MOR will also initiate a Phase 2 study in lower-risk myelodysplastic syndrome, in 2024. These phase 2 studies will inform further Phase 3 development plan. However, considering MOR's current cash runaway, MOR's success is dependent on pelabresib approval in frontline myelofibrosis.
Overview of the rest of the pipeline
I believe the major short/medium-term growth driver for MOR is approval of pelabresib. Hence the focus of this article. However, it is worth briefly discussing the rest of the pipeline.
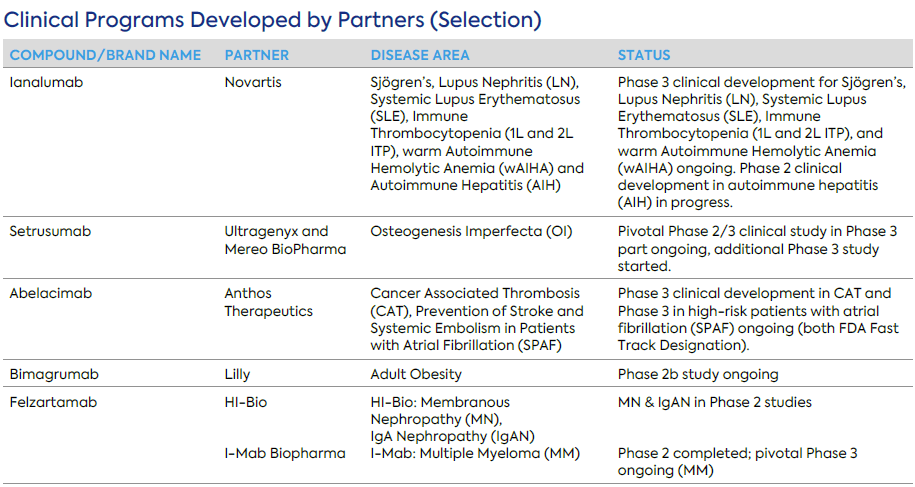
MOR has several partnered programs. A selection of late-stage partnered programs is listed in the table below, but there are several additional partnered programs in early to mid-stage research and development. MOR is entitled to milestone payments and royalties upon approval and commercialization of partnered assets. For example, from the licensing agreement with HI-Bio for MOR210 and felzartamab (granting HI-Bio worldwide right with the exception of Greater China for felzartamab and Greater China and South Korea for MOR210), MOR is eligible to receive up to $1B milestone payments plus tiered single to low double digit on net sales. Although partnered programs are not anymore the core business of MOR, at this point revenues from partnered programs are higher than Monjuvi revenues and these programs may offer potential upside and non-dilutive financing. Below are some recent highlights from partnered programs;
- Ultragenyx and Mereo BioPharma recently announced interim Phase 2 data demonstrating that setrusumab significantly reduced fracture rates in patients with Osteogenesis Imperfecta.
- Anthos Therapeutics revealed that its Phase 2 study of abelacimab in patients with Atrial Fibrillation was stopped early due to overwhelming positive results, highly significant reductions in bleeding events versus standard of care.
- On the other hand partnered programs have had big failures as well. For example GSK decided not to further explore otilimab after suboptimal results in a phase 3 studies (despite meeting the primary endpoint). Also, gantenerumab (partnered with Roche) failed in a phase 3 trial in early Alzheimer's diseases.
{kind=link}
Late-stage partnered programs (MOR Q3 2023 report)
MOR also has one approved product, Monjuvi, for which MOR has retained commercialization rights in the US. However, revenues from Monjuvi and partnered programs are still much lower than expenses (see next section). Specifically, Monjuvi sales face significant competition in the r/r DLBCL setting (current label), from CAR-T cell therapies, bispecific T cell engagers, as well as other antibody-based therapies. Notably, quarterly revenue from Monjuvi sales/royalties is relatively stable since Q4 2021. Potential label expansion to 1st-line DLBCL may considerably improve Monjuvi revenues, but topline results are expected in 2H 2025. MOR also aims for label expansion to r/r FL/MZL with topline expected in 2024, but the main upside would be expected from label expansion to frontline DLBCL.
Finally, beyond pelabresib, MOR is also developing tulmimetostat for solid tumors, which has been recently granted Fast Track Designation for "advanced, recurrent or metastatic endometrial cancer harboring AT-rich interacting domain containing protein 1A ( ARID1A ) mutations and who have progressed on at least one prior line of treatment". Notably, this is the third program (following Monjuvi and pelabresib) to have received Fast Track Designation. Tulmimetostat is a next-generation dual inhibitor of EZH2 and EZH1, designed to improve on first generation EZH2 inhibitors through increased potency, longer residence time on target and a longer half-life. Tulmimetostat is currently being evaluated in various tumors in an ongoing phase 1/2 study, with an estimated primary completion by the end of 2025.
Financials
MOR reported € 642.2 million in cash and other financial assets as of September 30, 2023. However, considering the high cash burn MOR has guided a runway into 2025, which is not re-assuring. Specifically, total revenue in Q3 was €63.8M (Monjuvi sales €21.5M, royalties €34M, licenses/milestones/other €8.3M), cost of sales €15.1M and total operating expenses were €99.7M (R&D €63.2M, SG&A €34.9M), resulting in an operating loss of €51M (€17M per month). Additional expenses resulted in a net consolidated loss of €119M.
To my understanding the guided cash runway does not take into account potential non-dilutive income from partnered programs (three of which are in the ph3 stage), although it is unclear if any significant milestone payments are anticipated during the projected runway. As far as pelabresib is concerned, MOR plans to commercialize it alone in US (considering the overlap with the Monjuvi infrastructure) but there is partnership potential outside US, which could also be a source of non-dilutive funding.
Risks
- The main short-term risks is FDA/EMA not accepting a regulatory submission based on available data. This would significantly impact MOR's valuation. Even after regulatory submission, delays in approval are possible.
- In high-risk patients TSS outcomes were significantly worse with pelabresib vs placebo, despite consistent benefit in SVR35. This inconsistency is a big concern that could affect the FDA/EMA decisions. Nevertheless, considering the consistent benefit in SVR35 and the small sample of high-risk patients (n=30) I agree with MOR that this finding is an "anomaly". Hopefully, there will be more clarity on this in the upcoming ASH presentation.
- A longer term risk is competition in a highly-competitive field (discussed in more detail above). At the moment, however, there seems to be very limited ph3-stage competition in the frontline, JAKi-naive setting (the target population of pelabresib). But more competition will likely emerge in this setting in the future.
- Failure of the rest of the pipeline.
Conclusion
Approval of pelabresib as frontline treatment in myelofibrosis would be a major success and growth-driver for MOR. Although I believe that totality of the evidence strongly supports pelabresib approval, the FDA/EMA may have a different opinion. MOR needs this win and a negative FDA decision would significantly impact MOR's stock price. Current cash runway is not enough for next catalysts if pelabresib fails.
Your feedback is appreciated
Please comment below if you have any feedback (positive or negative), if you spot any mistakes, or if you believe I missed something important in my analysis.
For further details see:
MorphoSys: A Buying Opportunity Following Mixed Phase 3 Results In Myelofibrosis