MCRB - Seres: VOWST Is A Great Product But Commercialization Prospects Unclear Due To Very High Price
2023-09-11 03:47:28 ET
Summary
- Seres Therapeutics launched VOWST for recurrent C. difficile infection in early June, in partnership with Nestle Health. VOWST represents a significant improvement over current standard of care.
- Considering high efficacy, safety and ease-of administration compared to alternatives, I am confident that both physicians and patients would prefer VOWST as a 1st-line option for treatment of recurrent CDIs.
- The major risk is the very high cost of VOWST (at $17.5K), meaning that insurance plans may cover VOWST only as 2nd-line (following failure of cheaper alternatives).
- Albeit promising, MCRB's pipeline is at a very early stage, and considering current cash balance and cash burn MCRB will soon need to raise cash unless VOWST sales pick up quickly.
Overview of the thesis
Approval of VOWST was a breakthrough both for Seres Therapeutics ( MCRB ) and for treatment of recurrent C. difficile infection ((CDI)), being the first commercial FDA-approved orally administered microbiome-based therapy in capsule form. VOWST is very effective in preventing recurrent CDI (better than most alternatives), is safe and is self-administered orally (vs need for office visit and enema/ colonoscopy/ intravenous infusion with alternative options). Taking price out of the equation VOWST could easily be the preferred 1st-line option by both physicians and patients for prevention of recurrent CDI. However, its very high price compared to alternative treatment options is concerning, as insurance companies may not cover VOWST as a 1st-line treatment before cheaper alternatives have been tried and failed. Seres will share profits and losses of VOWST with Nestle Health 50/50.
Current treatment options for recurrent C. difficile infection
Recurrent C. difficile infection requires repeat course of antibiotics (preferably fidaxomicin). Adjuncts to antibiotic therapy to reduce probability of recurrence include;
- Bezlotoxumab ; a monoclonal antibody that binds to C. difficile toxin B, and is given as a one-time infusion. Bezlotoxumab inhibits the binding of toxin B and prevents its effects on cells. Therefore, bezlotoxumab doesn't really target the disease at its root, it just prevents the toxicity of C. difficile -produced toxin. Bezlotoxumab is approved for patients with CDI recurrence within 6 months from the prior episode.
- Fecal microbiota transplantation ((FMT)). According to UpToDate authors, FMT is recommended for patients with a 4th or further CDI episode (i.e. 3rd or subsequent recurrence). Others , favor FMT for patients with a 3rd or further CDI episodes (i.e. 2nd or subsequent recurrence). Nevertheless, according to one study FMT may be cost-effective even for the 1st recurrence. FMT is usually administered via colonoscopy or retention enema, but is also available in capsule form. Limitations of FMT include: (1) safety concerns regarding donor stools (risk of pathogen transmission, including antibiotic-resistant bacteria), (2) scarcity of reliable access to therapy, (3) typical administration by colonoscopy/enema (requires office/hospital visit), (4) requires investment in human resources, equipment and space for the screening of donors, manufacturing of FMT, administration to patients, and quality oversight (thus FMT programs are often associated with larger academic hospitals and led by physician researchers).
- REBYOTA (a fecal microbiota rectal suspension), which was recently approved , and launched in February this year. REBYOTA is actually the first FDA-approved commercial microbiome-based treatment for recurrent CDI. REBYOTA is administered as a single enema (vs oral capsules with VOWST) and requires an office visit (in contrast to VOWST). In contrast to VOWST and FMT no preparation is necessary before administration. A limitation of REBYOTA is need for storage in an ultracold freezer, unless used within 5 days.
- VOWST ; Approved for recurrent CDI (including 1st recurrence). Treatment regimen includes 4 capsules once daily for 3 days. Patients also need to take 10 ounces (not much) laxative a day before VOWST initiation (vs no preparation necessary for REBYOTA). Patients must also fast for at least 8 hours before initiating treatment with VOWST.
Commercial fecal microbiota products (like VOWST and REBYOTA) that physicians prescribe to patients could improve access to therapy without the need to invest in human resources, equipment, and space. Unfortunately, comparative studies of VOWST with above options are currently lacking. Furthermore, studies on the efficacy of VOWST following failure of other options (e.g. after prior REBYOTA or FMT) are also lucking. Nevertheless, very high efficacy of VOWST in the phase 3 trial does not leave much room for improvement efficacy-wise.
Choosing between the above treatment options one should consider the following:
- efficacy; There is currently lack of studies directly comparing VOWST to above alternatives. Based on indirect comparisons (see table below) VOWST appears to be more effective than REBYOTA and bezlotoxumab, but likely not more effective compared to FMT.
- safety; Despite strict screening of donor and donor fecal specimens risk of pathogen transmission remains a concern with FMT . Although there are concerns for commercial products as well, the manufacturing process for VOWST minimizes risks for transmission of infectious agents.
- ease of administration; The major advantage of VOWST over above options is oral route of administration (vs enema/ colonoscopy/ intravenous) . Furthermore, patients can take VOWST at home (no need for office visit or hospital admission, in contrast to other options). On the other hand, patients do have to take a laxative a day before treatment and fast for at least 8 hours before treatment initiation (vs no preparation necessary for REBYOTA). However, I consider the latter a minor inconvenience compared to need for an office visit and enema/colonoscopy/intravenous administration.
- cost; VOWST is by far the most expensive option. I am not aware at present of any evidence that such a high price would be cost-effective (compared to bezlotoxumab, REBYOTA or FMT), nor has MCRB presented convincing such evidence to my knowledge. This could affect insurance coverage, resulting in VOWST being used as a 2nd (or more)-line treatment after failure of cheaper alternatives.
Taking cost out of the equation, I am confident that most physicians would recommend VOWST for treatment of CDI recurrences (including 1st recurrence) and most patients would prefer it to alternatives requiring office visit for administration by enema/colonoscopy (FMT, REBYOTA) or intravenously (bezlotoxumab). Therefore, the risk is not whether physicians prescribe VOWST but whether insurance plans will cover VOWST as a 1st-line option.
Finally, beyond already approved treatments, one should note that there are microbiome-based treatments under development for rCDI, including; VE303 (Vedanta Biosciences, which by the way also competes with MCRB on other indications under development) and CP101 by Finch Therapeutics (although the program has been discontinued ).
{kind=link}
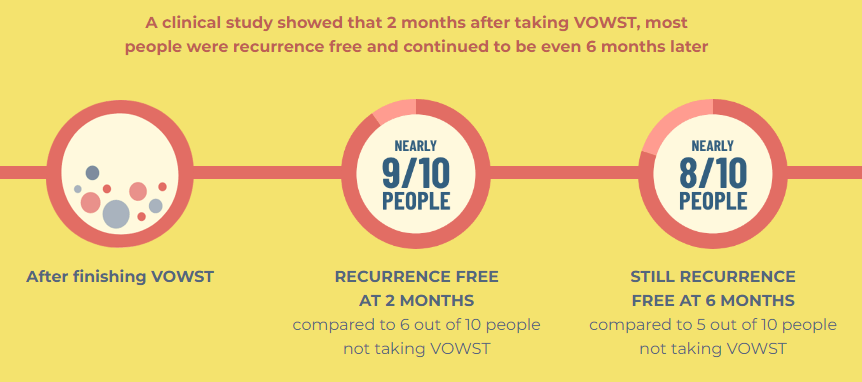
VOWST efficacy (VOWST website)
VOWST dosing regimen (doi: 10.1080/14787210.2023.2219894)
Comparison of available treatment options to reduce CDI recurrence
| Indication |
| Administration |
| Estimated cost ($) |
| % recurrence vs placebo in RCTs (relative risk) |
| VOWST |
| ?2 CDI episodes |
| Oral |
| 17,500 |
| 12% vs 40% (0.3) |
| REBYOTA |
| ?2 CDI episodes |
| Enema (single dose). Requires office visit |
| 6,750-11,250 |
| 29% vs 42% (0.7) |
| Fecal microbiota transplantation |
| ?3-4 CDI episodes |
| Administration by colonoscopy / retention enema / nasogastric tube / nasojejunal tube/ oral capsule. |
| 3,200-4,500 |
| 6.4-10% vs 33-46% (0.14-0.3) |
| Bezlotoxumab |
| ?2 CDI episodes (recurrence within 6 months) |
| Intravenous (single dose) |
| 2,364- 4,675 |
| 16-17% vs 26-28% (0.6) |
References: 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 . RCTs= randomized controlled trials
Note much lower relative risk for recurrence comparing VOWST to REBYOTA and bezlotoxumab. Also of note is that VOWST phase 3 was conducted in patients with >=3 CDI episodes (vs >=2 CDI episodes in REBYOTA phase 3 and >=1 CDI episodes in bezlotoxumab phase 3s), with 44% of VOWST-treated patients having >=4 prior CDI episodes. On the other hand, efficacy of VOWST does not appear to be better compared to FMT, although recurrences following FMT vary considerably in the literature, ranging from 0% to 24% (references; 1 , 2 , 3 ).
What does approval of REBYOTA and VOWST mean for FMT?
REBYOTA was the first fecal microbiota product approved by the FDA. At the same time of REBYOTA approval FDA also issued new guidance on use of FMT. Briefly , stool banks can continue to operate as long as they are compliant with the FDA’s IND requirements and health care professionals can still use appropriately screened donor stool for FMT procedures in patients with recurrent CDI whose symptoms do not respond to antibiotic therapies as long as informed consent is obtained from the patient.
Is VOWST cost-effective?
The burden of CDI in US is very high, affecting approximately 500,000 patients annually and resulting in 30,000 deaths per year. Recurrence after a 1st CDI episode is common, and following a recurrence the risk of further recurrences is much higher; up to 35% of index CDI will recur and of these up to 60% will further recur with multiple recurrences (although with currently available treatment options recurrence rates are much lower). Estimated total all-cause, direct medical costs during the 12-month period after an index CDI episode are high, starting at $71,980 for 1st CDI episode and ranging between $131,953 for patients with one recurrence to more than $200,000 in patients with three or more recurrences.
I am not aware of any published cost-effectiveness analysis on VOWST. Nevertheless, considering above costs associated with CDI recurrences and VOWST's efficacy, I am confident that VOWST is cost-effective when compared to no adjunctive treatment to reduce recurrence risk (I refer readers to the article by Clinically Sound Investor for more details on this). However, considering the several available options for management of patients with recurrent CDI one should consider the cost-effectiveness of VOWST to these approaches. Insurance companies are unlikely to cover VOWST as a first-line option when much cheaper alternatives are available, unless VOWST is cost-effective. Unfortunately, I am not aware currently of a cost-effectiveness analysis comparing VOWST to alternative options (including FMT, REBYOTA and bezlotoxumab) nor has MCRB provided such data to my knowledge.
View of the medical community on VOWST
According to UpToDate authors the following are stated on VOWST and REBYOTA ( article 1 , article 2 ):
we await more data comparing them to other sources of FMT and bezlotoxumab before adopting their use
It remains to be seen how this new fecal microbiota oral capsule will compare with traditional methods of fecal microbiota transplantation, the recently approved fecal microbiota rectal suspension, and bezlotoxumab, and whether it is a cost-effective preventive tool for CDI recurrences
Many clinicians worldwide use UpToDate to guide their everyday clinical practice. Therefore, the opinion of UpToDate authors is concerning and surprising to me. Personally, as described above, I believe VOWST to be a very good 1st-line option considering proven efficacy, safety and ease of treatment, the only real competitor being traditional FMT (especially in capsule form) where available.
In another recent publication authors highlight the much higher cost of VOWST compared to alternatives (including FMT and REBYOTA), as well as the lack of published cost-effectiveness analyses considering VOWST in the treatment algorithm. In another publication author highlight advantages of VOWST (safe, effective, oral route of administration, self-administered without need for office-visit or hospitalization), but acknowledge that "more information on indirect costs is needed". Finally, according to a survey by MCRB 75% of physicians would definitely (22%) or probably (52%) prescribe VOWST.
To sum up, healthcare practitioners' opinions on VOWST differ on the role of VOWST over alternative. Importantly, even if the healthcare provider prescribes VOWST it doesn't matter if insurance won't cover it as 1st line.
Is the market potential of VOWST overestimated?
According to a meta-analysis , a 1st CDI recurrence affects about 70,000 patients per year in the US (31-35K community-associated CDI, 38-58K health-care associated CDI). According to other estimates, recurrences (total, not just 1st recurrence) account for 75,000 to 175,000 additional cases of CDI per year. According to MCRB's company presentation the estimated number of CDI recurrences for 2023 is 156,000 cases. Considering VOWST's price ($17,500) this means a market size potential of >$1B just considering 1st recurrences, and up to $3B considering all recurrences.
Let's now consider a worst-case scenario where all 1st CDI episodes are treated with fidaxomicin (the treatment option with lowest recurrence rate) and insurance companies require patients to be treated with another option before being eligible for treatment with VOWST (in other words patients would be eligible for VOWST only for 2nd and subsequent recurrences). At least 300K US patients (500K total minus 175K recurrences, based on above estimation) have a first CDI per year. Even if all patients were treated with fidaxomicin, there is still a 11-13% probability of recurrence risk, meaning 30K patients with a 1st CDI recurrence per year. If all 1st recurrences were treated with alternative options there is still a 15-20% (references; 1 , 2 , 3 ) risk of 2nd recurrence, meaning 3-8.7K patients, i.e. a total market size potential of just $52M-$152M per year.
I believe the true market potential is somewhere in between the above 2 scenarios, but likely closer to the latter than the 1st scenario. MCRB expects coverage policies to begin to be issued during H2 2023, so there should be news soon. Finally, it is important to note again that profits from VOWST are shared 50-50 with Nestle.
Brief overview of the rest of the pipeline
Although the focus of this article is on VOWST, it would be unfair for MCRB not to recognize the potential of its pipeline, despite being early stage. The most advanced candidate is SER-155 which is currently being developed for prevention of infections and acute GVHD in allo-HSCT patients. MCRB is also researching future development plans for ulcerative colitis. Finally, there are preclinical programs; one targeting antimicrobial-resistant infections in immunocompromised patients and the other targeting oncology (aiming to modulate host immunity/inflammation to improve response and tolerability of cancer treatments).
SER-155 is an investigational, oral, 16 strain, cultivated microbiome therapeutic designed to prevent colonization and reduce the abundance of ESKAPE pathogens ( Enterococcus faecium , Staphylococcus aureus , Klebsiella pneumoniae , Acinetobacter baumannii , Pseudomonas aeruginosa , and Enterobacter species) in the GI tract to reduce the risk of enteric driven bloodstream infections and other downstream consequences, such as GvHD, in patients receiving allo-HSCT. Promising results were recently reported from its ongoing phase 1b study, showing the successful engraftment of SER-155 bacterial strains and a substantial reduction in the cumulative incidence of pathogen domination. Results of the second cohort (randomized, double-blinded placebo-controlled), including clinical outcomes, are anticipated mid-2024.
In my opinion the potential of SER-155 (or other next-generation microbiome-based product) is far greater and unlikely to be limited just to allo-HSCT patients, if proven to effectively prevent/reduce colonization/infection by resistant bacteria. Antibiotic-resistant bacteria is a major emerging threat resulting in increased mortality and costs. Furthermore, emergence of resistance by far outpaces development of new antibiotics, the result being emergence of bacteria resistant to all currently available antibiotics. A treatment option that can reduce the abundance (or even better achieve decolonization) of antibiotic-resistant pathogens would be a big deal. Of note VE707 of Vedanta Biosciences is a big competitor on this indication, but at an earlier stage compared to MCRB.
Financials
As of June 30, MCRB reported about $230M cash and cash equivalents. Total operating expenses were about $77M (R&D $46M including $11.0M of commercial manufacturing costs for VOWST, G&A $28M). At this rate of cash burn MCRB will soon need to raise cash unless VOWST sales pick-up quickly. MCRB is also entitled to three additional tranches of its debt facility which are however dependent on VOWST success; two $45M tranches each based upon the achievement of certain applicable VOWST sales targets, plus an additional $50M at Oaktree's discretion.
Since VOWST was launched in early June, Q2 sales were low as expected ($1.2M). Nevertheless, demand was promising (610 completed prescription enrollment forms) proving the interest of physicians in VOWST. Coverage policies are anticipated to start being issued during the next months. The fact that 57% of the 282 patients were reimbursed is promising. Approval of a new technology add on payment or in-tap for VOWST when used for patient's treated in the inpatient setting (meaning that hospitals will receive extra payment for any Medicare patients treated with VOWST in the inpatient setting next year) is also promising.
Risks to the thesis
Although I tend to be optimistic considering significant advantages of VOWST over alternatives, a major risk is that insurance reimbursement policies will be unfavorable (see "worst-case scenario" discussed above) due to the very high cost of VOWST compared to alternative options. Underwhelming VOWST sales will mean that MCRB won't gain access to the rest of the tranches of its loan facility and will have to do a dilutive cash raise.
Longer term there is risk from competition, e.g. Vedanta Biosciences' VE303 which has showed similar efficacy and could reach the market in a few years.
Conclusion
Taking cost out of the equation and considering very high efficacy, safety and being logistically (oral, self-administered) an easier treatment option I feel confident that most physicians would recommend VOWST as a 1st-line option for treatment of recurrent CDI and patients would be more satisfied with this option. Furthermore, considering burden and costs of CDI recurrences, I am confident that VOWST is cost-effective compared to no treatment. The big question is whether VOWST is cost-effective compared to alternatives (bezlotoxumab, FMT, REBYOTA). The very high price of VOWST compared to alternatives may severely limit its commercial potential if insurance companies do not cover its use as first line treatment. Therefore, pending more news on VOWST rollout and coverage commercial prospects remain uncertain. Nevertheless, my sentiment is positive and taking all above parameters into consideration I tend to be optimistic that VOWST rollout will eventually be successful.
Your feedback is appreciated
Please comment below if you have any feedback (negative or positive), if you spot any mistakes or if you believe I missed something important in the article.
For further details see:
Seres: VOWST Is A Great Product But Commercialization Prospects Unclear Due To Very High Price