CRNX - Crinetics Pharmaceuticals And Its Value Proposition In Acromegaly
2023-05-25 12:25:15 ET
Summary
- Crinetics Pharmaceuticals, Inc. is developing an oral nonpeptide drug for acromegaly patients.
- The drug is claimed to have advantages over injectable and oral somatostatin analogues.
- A phase 3 trial will establish that claim more strongly.
Crinetics Pharmaceuticals, Inc. ( CRNX ) develops GPCR-targeted (GPCR= G-protein coupled receptors) oral small molecules for endocrine diseases and endocrine-related tumors. Its pipeline looks like this:
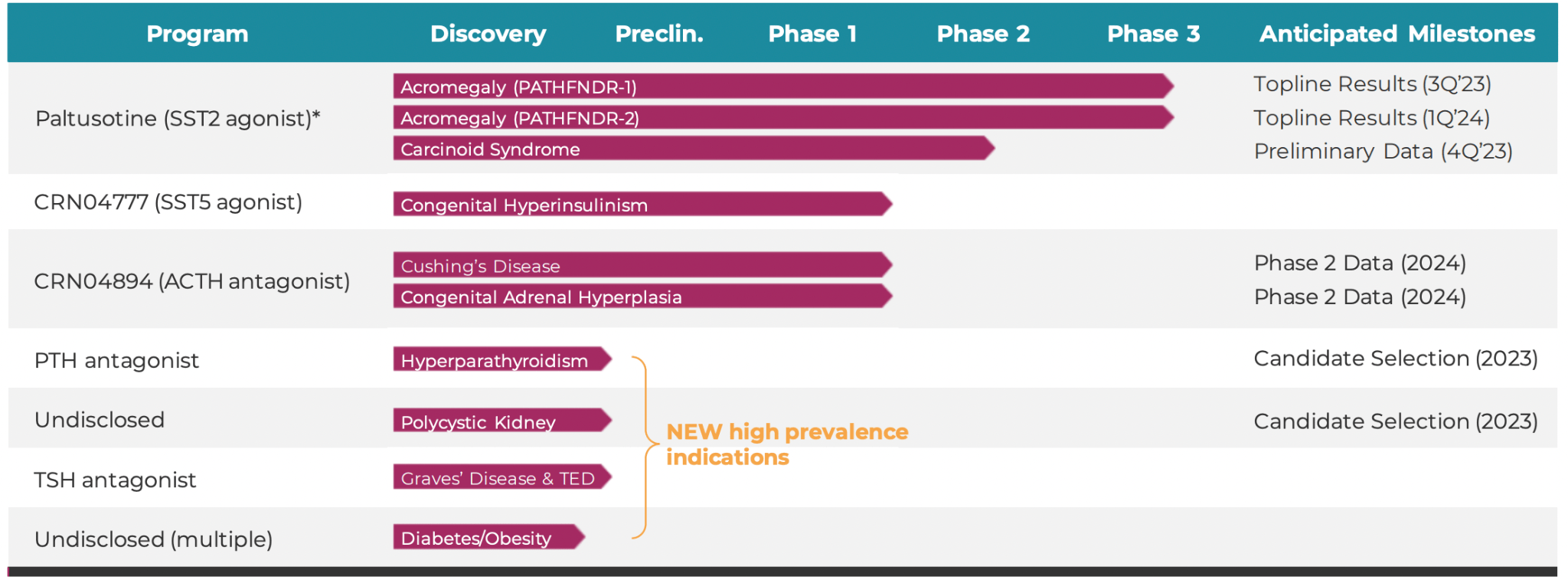{kind=link}
Lead candidate Paltusotine is an oral, selective, nonpeptide, somatostatin receptor type 2 (SST2) agonist designed for the treatment of acromegaly, where it is in a phase 3 trial. It is also in a phase 2 trial in carcinoid syndrome. In acromegaly, currently available peptide drugs need painful monthly or daily injections, or a strict twice-a-day oral dosing regimen. Current somatostatin peptide drugs often fail to halt disease progression.
Acromegaly as we know it is abnormal growth in humans, including arms, legs and facial features. It is caused by the secretion of excess growth hormones by a benign pituitary tumor, technically called an adenoma. This also causes excess IGF-I secretion in the liver. Somatostatin Receptor Ligands (SRLs) inhibit GH secretion.
The primary goal of treating acromegaly is to normalize GH and IGF levels. Current primary approach to treatment begins by surgically removing the offending adenoma using a transsphenoidal approach, i.e. surgery through the nose . If the tumor is invasive, or the lesion is greater than 4 cm, surgery often does not work alone. Even otherwise, GH levels are not normalized post-surgery in about 30% of patients. This occurs generally when the entire tumor cannot be removed. In these cases, radiation, and medical therapies, are required. To put all of that in technical terms :
However, resection leads to remission in only about half of patients, and many require adjuvant pharmacotherapy to normalize GH and IGF-I levels.
The aim of these drugs is also to lower levels of GH and IGF-I. There are three main classes of drugs - somatostatin analogues, dopamine agonists and growth hormone antagonists. SSA therapy works because natural somatostatin works through a negative feedback mechanism with GH. When GH is more, the body secrets somatostatins to control and reduce GH. However, when there’s just too much GH for the body to cope up, artificial somatostatins, or somatostatin analogues, can be useful. Octreotide and lanreotide are the two main SSAs. These are usually given as a monthly injection to your buttocks (the gluteal muscles), in a hospital setting or by a professional. Mycapssa is an oral version of octreotide, but it is not as effective as octreotide, and requires two daily dosings with fasting 1 hour before or 2 hours after dosing. Although oral SRL developers claim non-inferiority, in practice, iSRLs (Injectible SRLs) are preferred. About mycapssa’s need as an oral alternative minus harmful effects of injectable but efficacious iSRLs:
To this end, a twice-daily oral formulation of octreotide was approved in the United States in 2020, based on a phase 3 study that showed maintenance of normalized IGF-I in 58.2% of patients with acromegaly who switched from long-acting peptide injectable SRL to oral octreotide vs 19.4% for those who switched to placebo ( P = .0079).
It is in this setting that we need to understand Paltusotine. Paltusotine is an oral SRL. Unlike Mycapssa, it is not a peptide. The company claims that this gives it some advantages.
A phase 2 study called ACROBAT had the objective of evaluating change in IGF-I levels in patients switched from octreotide long-acting release or lanreotide depot monotherapy to paltusotine. However, this was an open label, nonrandomized study where patients simply switched from these iSRLs to paltusotine.
Data :
In group 1 (n = 25), IGF-I and GH showed no significant change between SRL baseline and end of paltusotine treatment at week 13 (median change in IGF-I = ?0.03×upper limit of normal [ULN]; P = .6285; GH = ?0.05 ng/mL; P = .6285). IGF-I and GH rose significantly in the 4 weeks after withdrawing paltusotine (median change in IGF-I = 0.55×ULN; P < .0001 [median increase 39%]; GH = 0.72 ng/mL; P < .0001 [109.1% increase]). No patients discontinued because of adverse events (AE); no treatment-related serious AEs were reported.
Not a lot of conclusions can be drawn from here that cannot be countered. So patients first took iSRLs, then switched to paltusotine, and then had a washout period. IGF/GH levels were maintained during the first two periods, and dropped significantly in the last period. What does that tell you? The bull case is that paltusotine was able to maintain GH/IGF levels as well as iSRLs. The bear case is that iSRLs had a longer-than usual duration of treatment, or otherwise supported the paltusotine dosage. The only way to decide between the two scenarios is to put them in two separate, randomized arms, and have them go at it. (note that analysis was performed on this exact question, and plasma concentrations of these iSRLs were found to be at pretrial levels at week 13. However, note that there was some overlap between plasma concentration testing times that were done after baseline, and paltusotine dosage. I mean, up to week 7 of paltusotine therapy, there was presence of octreotide in serum). The main limitation of this phase 2 study, as I see it, is that there were no acromegaly patients without prior experience of injectable SRL usage, or usage of other pharmacotherapy treatment options.
Another limitation is the short duration, for which a long duration open label extension study was performed. This study saw that paltusotine lowered and maintained IGF-1 at levels comparable to prior injected SRL therapy for up to 103 weeks, and that at Week 52, thirty-two (88.9%) of the 36 respondents preferred once daily paltusotine treatment.
I discussed the bull/bear scenarios and why it is necessary to pit the two competitors against each other in a single trial. The two phase 3 PATHFNDER studies are not exactly doing that, however, they have a more clinically defined reduction in IGF levels as their primary endpoints. The main difference between the two trials is that the first trial will have patients who were on stable doses of octreotide, while the second trial will have untreated patients. That last option is as good as it gets here, versus the gold standard of such clinical trials, putting both comparators in active arms and letting them prove themselves.
Paltusotine will compete with both injectable SRLs like octreotide, and mycapssa and its variants. I can appreciate the use of placebo in disease settings without clear competitive treatment options, but here, where there are clear competitors, acceptance of the new therapy by doctors will probably need them to be compared directly. Without such direct comparison, the FDA may approve the therapy, however, the medical community may not, unless the differences between study data and historical data are very starkly defined.
Financials
Crinetics Pharmaceuticals, Inc. has a market cap of $1.22bn and a cash balance of $296mn. Research and development expenses were $38.5 million for the three months ended March 31, 2023, while general and administrative expenses were $12.2 million. At that rate, they have a cash runway to the end of 2024.
Bottom Line
Crinetics Pharmaceuticals, Inc. is about quite a bit more than acromegaly. There was a radiotherapy unit which they spun out into a standalone company. There is the rest of its pipeline, especially Hyperinsulinism, which was put on a hold on its phase 2 IND in November. I haven’t discussed all of that, focusing mainly on acromegaly and paltusotine’s scientific value proposition. I think Crinetics Pharmaceuticals, Inc. is an interesting company doing good medicine, and I would like to see more.
For further details see:
Crinetics Pharmaceuticals And Its Value Proposition In Acromegaly