CRNX - Evaluating Crinetics' Oral Long Shot For Acromegaly
2023-03-06 10:13:25 ET
Summary
- Crinetics Pharmaceuticals develops therapeutics for endocrine diseases and tumors. Its lead drug candidate, paltusotine, is undergoing two Phase 3 trials for acromegaly treatment.
- In acromegaly, the excessive production of growth hormone and insulin-like growth factor 1 [IGF-1] causes several symptoms, including enlarged facial features, enlarged hands and feet, joint pain, and fatigue.
- Paltusotine is a highly selective oral drug that activates somatostatin receptor subtype 2, decreasing levels of growth hormone and insulin-like growth factor 1 [IGF-1].
- In the Phase 2 ACROBAT program, 47 acromegaly patients switched from an injected somatostatin analog to oral paltusotine and the study found that it was able to maintain IGF-1 levels at Week 13 with some variability.
- Crinetics' Phase 3 results for acromegaly will impact its valuation, but any doubts about paltusotine's relative efficacy could lead to a negative outcome. With its less efficient oral delivery, it is currently a "Sell," but still worth monitoring.
Introduction
Crinetics Pharmaceuticals ( CRNX ) is a clinical-stage biotechnology company that develops therapeutics for endocrine diseases and endocrine-related tumors. Its lead drug candidate, paltusotine , is a highly potent somatostatin receptor subtype 2 [SST2] agonist currently undergoing two Phase 3 trials for the treatment of acromegaly, a rare hormonal disorder caused by the overproduction of growth hormone.
Financials
In its financials , Crinetics reported research and development expenses of $130.2 million for the full year ended December 31, 2022, primarily related to clinical and nonclinical activities for paltusotine, CRN04777, CRN04894, and preclinical programs. General and administrative expenses were $42.4 million for the same period, mainly due to personnel costs. Revenues were $4.7 million for the full year, primarily consisting of license revenue recognized from the license agreement entered into with Sanwa in February 2022. As of December 31, 2022, Crinetics had $334.4 million in unrestricted cash, cash equivalents, and investments, which it expects to fund its current operating plan through 2024.
Paltusotine: A Highly Selective SST2 Agonist with Potential for Acromegaly Treatment
Paltusotine is a drug that activates the somatostatin receptor subtype 2 [SST2] in the body. It is extremely selective for SST2, meaning it has a high affinity for this receptor compared to others. Paltusotine has been shown to decrease the levels of growth hormone and insulin-like growth factor 1 [IGF-1] in healthy volunteers. Additionally, it has a high bioavailability, meaning it can be taken orally and easily absorbed by the body.
This is particularly useful for acromegaly as the disease is caused by excess growth hormone production in the pituitary gland. By activating SST2, paltusotine can effectively reduce the levels of growth hormone and insulin-like growth factor 1 in the body, which can alleviate symptoms of acromegaly. The high oral bioavailability of paltusotine also makes it a convenient treatment option for patients, as they can take it orally, once daily, rather than having to receive injections.
Understanding the Goals and Treatment Algorithm for Acromegaly
In acromegaly, the excessive production of growth hormone and insulin-like growth factor 1 [IGF-1] causes several symptoms, including enlarged facial features, enlarged hands and feet, joint pain, and fatigue.
The goals of therapy for acromegaly include lowering IGF-1 concentration, controlling adenoma size, improving symptoms, reversing metabolic abnormalities, and lowering serum GH concentration. Biochemical goals include lowering serum GH concentration to <1 mcg/L and lowering IGF-1 concentration to within the normal range. Treatment can lead to the regression of soft tissue overgrowth, improvement of metabolic abnormalities, and a return to normal life expectancy. Another goal is to alleviate symptoms due to the adenoma without causing hypopituitarism.
The current standard of care for acromegaly is transsphenoidal surgery to remove the tumor of the pituitary gland. If patients remain symptomatic or continue to have abnormal serum IGF-1, medical therapy is indicated and described below.
| Treatment Algorithm for Acromegaly |
|---|
| For patients with abnormal serum IGF-1 and moderate symptoms after surgery but who do not need repeat surgery, medical therapy with a long-acting somatostatin analog or pegvisomant is suggested. |
| If serum IGF-1 levels are not normalized after surgery, medical therapy with either a somatostatin analog or pegvisomant is suggested. |
| In patients with only modest biochemical abnormalities and mild symptoms, a trial of cabergoline is suggested. |
| Stereotactic radiation therapy is suggested if medical therapy is ineffective or not tolerated, or if there is an adenoma increasing in size despite medical therapy. |
Medical therapy may be the preferred initial treatment option for patients who are not suitable candidates for surgery, who do not wish to undergo surgery, or for whom the tumor cannot be completely removed.
Exploring Current Medical Therapies for Acromegaly: A Focus on Somatostatin Analogues
In order to provide a better understanding of the competitive landscape for paltusotine, it is important to delve into the details of current medical therapies. One such therapy is somatostatin analogs, including Octreotide and Lanreotide, which have higher potency and longer plasma half-life than native somatostatin, making them more effective at inhibiting growth hormone [GH] secretion. These analogs bind to specific receptors for somatostatin and can cause pituitary adenoma shrinkage in some patients, although the exact mechanism is not fully understood.
In the body, there is an inverse relationship between GH and somatostatin (also known as growth hormone-inhibiting hormone or GHIH). The pituitary gland releases GH, which stimulates growth and cell reproduction in humans and animals. However, in the case of acromegaly, excess GH is produced, leading to abnormal growth. Somatostatin, on the other hand, inhibits the release of GH from the pituitary gland by binding to specific receptors, reducing the production and release of GH. This negative feedback mechanism helps regulate GH levels in the body.
However, somatostatin analogs like Octreotide have a significant disadvantage in that they must be administered subcutaneously three times a day for two weeks with Sandostatin Injection, followed by an intragluteal dose of 20 mg every four weeks for three months.
Mycapssa is an oral formulation of octreotide that was approved for the management of acromegaly in 1988. It utilizes a transient permeability enhancer to enable gastrointestinal absorption and is indicated for long-term maintenance therapy in patients who have responded to and tolerated treatment with either octreotide or lanreotide. In a study of 155 patients previously controlled on injectable somatostatin analogs, Mycapssa was found to be less effective than long-acting injectable preparations. However, 65% of the patients achieved the primary endpoint of GH/IGF-1 control (IGF-1<1.3×ULN), and the adverse event profile was similar to that of injectable somatostatin analogs. Oral octreotide is seldom used due to its perceived lower effectiveness in comparison to subcutaneous formulations.
Crinetics' Paltusotine: Promising Oral Treatment for Acromegaly Patients Previously Receiving Somatostatin Analog Injections
Crinetics' goal is to offer an oral treatment alternative that is just as effective for individuals with acromegaly who currently need to receive injections of somatostatin analogs. In a Phase 2 program called ACROBAT, Crinetics evaluated paltusotine in acromegaly patients who had previously received injections of either octreotide or lanreotide monotherapy. The first trial, called Edge, was an open-label study that evaluated the effects of paltusotine on patients whose insulin-like growth factor 1 levels were not biochemically controlled by octreotide or lanreotide alone. The second trial, called Evolve, was a double-blind, randomized, placebo-controlled trial in patients whose insulin-like growth factor 1 levels were biochemically controlled by octreotide or lanreotide monotherapy.
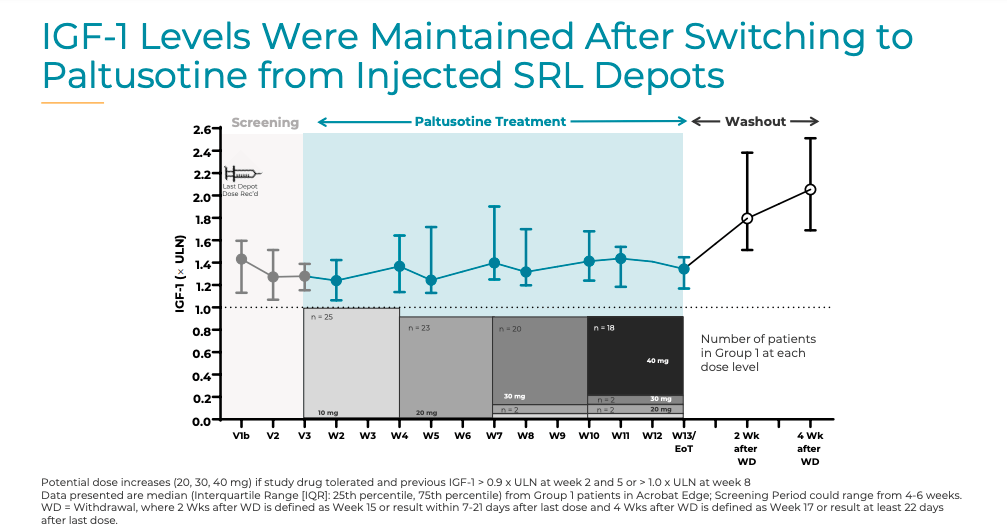
In October 2020, Crinetics announced positive top-line results from the ACROBAT program. In the Edge trial, 47 acromegaly patients were switched from an injected somatostatin analog to oral paltusotine. The study found that paltusotine was able to maintain insulin-like growth factor 1 levels at Week 13. During the four-week washout period, patients experienced a significant (>20%) and rapid (within two weeks) increase in insulin-like growth factor 1 levels from baseline. These results demonstrated the magnitude of therapeutic activity of oral paltusotine in acromegaly patients. In Group 1 (n=25), there was no significant change in IGF-I and GH levels between SRL baseline and the end of paltusotine treatment at week 13 (median change in IGF-I = -0.03×ULN, P = 0.6285; GH = -0.05 ng/mL, P = 0.6285). 87% of the patients (20 out of 23) who completed the dosing period were able to achieve IGF-1 levels at the end of treatment that were equal to or less than 20% of their baseline levels. However, there was a significant rise in IGF-I and GH levels in the four weeks after withdrawing paltusotine (median change in IGF-I = 0.55×ULN, P < 0.0001 [median increase 39%]; GH = 0.72 ng/mL, P < 0.0001 [109.1% increase]). No patients discontinued the trial due to adverse events, and no treatment-related serious adverse events were reported.
The enrollment in Evolve was terminated early, and data from the reduced sample size was combined with data from the Edge study for post-hoc analyses.
Crinetics' Phase 3 Trials of Paltusotine for Acromegaly: PATHFNDR-1 and PATHFNDR-2
The Phase 3 development program for paltusotine consists of two placebo-controlled trials: PATHFNDR-1 and PATHFNDR-2 . PATHFNDR-1 is a nine-month trial for patients with average IGF-1 levels less than or equal to 1.0 times the upper limit of normal and who are on stable doses of SRL monotherapy. PATHFNDR-2 is a twenty-four-week trial for untreated patients with elevated IGF-1 levels, stratified into three groups. The primary endpoint for both trials is the proportion of patients with IGF-1 ? 1.0 × ULN at the end of the treatment period on paltusotine as compared to placebo. Enrollment for PATHFNDR-1 was completed in 2022, and top-line data is expected in Q3 2023. Enrollment for PATHFNDR-2 is ongoing, and top-line data is expected in Q1 2024. If successful, these trials could support marketing applications for paltusotine for all acromegaly patients who require pharmacotherapy, including untreated patients and those switching from other therapies. An NDA submission is anticipated in 2024.
Paltusotine Faces Challenges in Achieving Phase 3 Endpoint of IGF-1 Levels Compared to Phase 2 Exploratory Endpoint
Paltusotine may have a more difficult time achieving the Phase 3 endpoint of IGF-1 levels ? 1.0 times the upper limit of normal compared to the Phase 2 exploratory endpoint of achieving IGF-1 levels at the end of treatment that were equal to or less than 20% of the baseline levels (20/23, 87%).
The Phase 3 endpoint requires more specific and stringent targeting of IGF-1 levels (compared to Mycapssa's IGF-1 < 1.3×ULN endpoint), aiming to bring/maintain the levels down to a very low range. In contrast, the Phase 2 exploratory endpoint had a wider range of acceptable IGF-1 levels that were still considered effective.
Additionally, the Phase 3 endpoint is likely to be more clinically meaningful and relevant for patients as it reflects the desired therapeutic effect of bringing IGF-1 levels to a safe and effective range.
Therefore, the Phase 3 endpoint of IGF-1 levels ? 1.0 times the upper limit of normal may pose a greater challenge for paltusotine to demonstrate efficacy, and the results may have a greater impact on the drug's regulatory approval and clinical use compared to the Phase 2 exploratory endpoint.
Comparing the Theoretical Efficacy of Paltusotine and Octreotide in Suppressing Growth Hormone and IGF-1 Secretion in Acromegaly Patients
Overwhelmingly positive Phase 3 trial results for paltusotine could establish it as a desired treatment option for acromegaly patients, offering benefits like easier dosing while maintaining similar effectiveness in certain patient groups. However, achieving this will not be without challenges, and there may be lessons to learn from Mycapssa's lack of success.
Paltusotine and octreotide both act by inhibiting growth hormone secretion through binding to SST2 receptors in the pituitary gland. However, the efficacy of subcutaneous octreotide in suppressing GH and IGF-1 levels is attributed to the drug's direct and consistent delivery to the bloodstream, leading to rapid and potent suppression. As an oral medication, paltusotine needs to pass through the digestive system before reaching the bloodstream, which can result in lower bioavailability and less consistent absorption, reducing its effectiveness in suppressing GH and IGF-1 secretion.
Octreotide is a non-selective somatostatin analog that can bind to multiple subtypes of somatostatin receptors , including SST2, SST3, and SST5, allowing for a more comprehensive suppression of GH and IGF-1 secretion. In contrast, paltusotine is a selective SST2 agonist, limiting its efficacy in suppressing GH and IGF-1 secretion, especially if other receptor subtypes are involved in the regulation of these hormones. While SST2 receptors are the most abundant subtype in the pituitary gland, other subtypes are also present and can contribute to the overall regulation of GH and IGF-1 secretion.
Octreotide's ability to target multiple receptor subtypes means it can exert a more widespread effect on GH and IGF-1 secretion, potentially achieving a more complete suppression of these hormones, while paltusotine's selectivity may limit its efficacy in controlling GH and IGF-1 levels. Although paltusotine may offer advantages such as more convenient dosing, it may not achieve the same level of efficacy as subcutaneous octreotide in controlling GH and IGF-1 levels in acromegaly patients.
The figure below exhibits signs of variability even with a cursory glance.
{kind=link}
Crinetics
In order for paltusotine to be deemed as effective as subcutaneous somatostatin analogs, it will need to significantly reduce variability. Although Mycapssa was able to achieve GH/IGF-1 control in 65% of patients, it is still regarded as inferior to subcutaneous formulations. Paltusotine will need to attain much better results than this to persuade clinicians and patients of its comparable efficacy and relevance in the market.
Conclusion
Certain medications demonstrate greater effectiveness when administered subcutaneously, particularly in cases where the disease demands it. For example, diabetes, another endocrine disorder that is a result in negative feedback dysfunction, necessitates insulin to be optimally delivered subcutaneously to regulate blood sugar levels. Subcutaneous injection ensures a controlled and predictable delivery of insulin into the bloodstream. Acromegaly, for instance, requires a controlled and predictable suppression of growth hormone, which can be best achieved through subcutaneous injection.
If paltusotine can prove its efficacy convincingly, it has the potential to become a blockbuster drug. However, if it fails to do so, it may not be more relevant than Mycapssa. In my view, due to its selectivity and oral route of administration, which involves passing through the gastrointestinal tract before reaching its target, paltusotine is likely to result in variability among acromegaly patients, thereby reducing its overall relative efficacy.
Crinetics is currently also testing paltusotine for the treatment of carcinoid tumors (Phase 2), which requires similar treatments to acromegaly. The company's other prospects are either preclinical or Phase 1. Later this year, investors can expect Phase 3 results for acromegaly, which will significantly influence Crinetics' valuation. While Crinetics may successfully achieve primary and secondary endpoints, justifying FDA approval, any doubts about paltusotine's relative efficacy may lead to a similar fate as Mycapssa. Since paltusotine's oral delivery may be less efficient than subcutaneous somatostatin analogs for acromegaly, the most probable outcome is a net negative for Crinetics. Therefore, Crinetics is currently a "Sell," but it is a story worth keeping an eye on.
For further details see:
Evaluating Crinetics' Oral Long Shot For Acromegaly