VERA - Chinook Therapeutics: Best Biotech For Kidney Disease Exposure With Catalysts
Summary
- 2023 should be a year of progress on kidney disease, with multiple catalysts lined up from multiple companies.
- Chinook Therapeutics, Inc. has the best risk-reward based on: i) valuation; ii) diversity of pipeline (ERA and anti-APRIL); and iii) clear catalyst in Q3 2023 (phase 3 ALIGN data of Atrasentan).
- We like both Atrasentan and BION-1301’s mechanism of action and clinical/pre-clinical data so far.
- KDNY has a robust cash runway until 2025.
Background & KDNY's platform technology
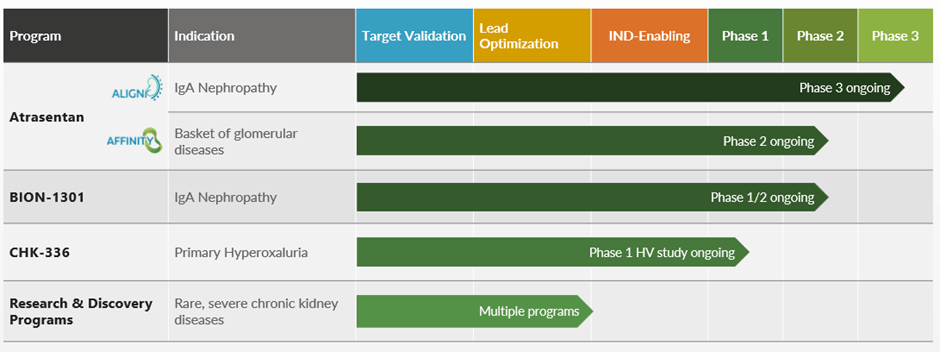
Chinook Therapeutics, Inc. (KDNY) is developing two therapies targeting IgA nephropathy that will play a key role in IgA Nephropathy. Atrasentan is an endothelin receptor antagonist, which treats IgAN through the hemodynamic mechanism of action and also reduces fibrosis (the endothelin system has been implicated in the deposition of collagen and fibrosis and podocyte production).
Pathophysiology of IgAN (Company)
We believe there is robust pathological rationale around the ETa receptor's role in: i) vasculature; ii) podocyte production; iii) renal tube (tubulointerstitial fibrosis); iii) mesangium (mesangial proliferation and matrix accumulation, glomerulosclerosis); and iv) inflammation. These are key components of proteinuria, inflammation, and fibrosis that plays a key role in CKD progression. Even though Atrasentan is not modulating the immune system, we see it being used in combination with the current standard of care RASi (ACEi and ARBs) to treat mild-moderate patients before moving into immune system modulation therapies that target B-cell or complement systems.
BION-130 is an immune system modulation anti-APRIL antibody that we believe will be positioned after ACEi+ERA in patients with consistent proteinuria.
The anti-APRIL pathway targets the "core" of IgAN disease, the production of pathological Gd-IgA autoantibodies that start the immune complex and inflammation leading to ESRD. This means that BION-1301 will be a disease-modifying treatment, unlike ERAs or RASi which primarily treat the disease primarily through a hemodynamic mechanism of action. We expect a better ability in stabilizing the eGFR of IgAN patients (long term) with BION-1301. We believe ACEi/ARB, ERA, B-cell modulators, steroids, and complement inhibitors all have a place in IgAN because they all work complementarily. APRIL therapy blocks B cell production of pathogenic IgA, complement blocks inflammation in the kidney, and ERA is known to have a generic effect or reduce fibrosis, on top of some hemodynamic mechanisms of action. We think ACEi/ARB's key mechanism of the action revolves around the hemodynamic mechanism of action, reducing pressure in the kidney and some attributes of the drug reducing albumin absorption in the proximal tube.
Of note, if complement inhibitors are approved, we expect them to compete with steroids, like Tarpeyo from Calliditas Therapeutics AB (publ) ( CALT ) as they mainly target the same "inflammatory" aspect of IgAN. Multiple combination therapies will emerge, and with more data published during 2023, we will get a better sense of how these agents will be used in combination.
{kind=link}
Approval of Atrasentan is expected in 2024/2025 based on phase 3 ALIGN data
{kind=link}
We note that FDA is accepting proteinuria ((UPCR)) as a "reasonably appropriate surrogate endpoint" for accelerated approval in IgAN disease. Based on this, sponsors (biotech companies) have started designing their trials around this endpoint. Although, we note that the drug should show clear eGFR separation with a placebo for full approval. Keeping this regulatory shift that happened during the last 5 years, KDNY is targeting to receive approval based on proteinuria as an endpoint where we expect the company to publish top-line proteinuria data of its ALIGN trial during Q3 2023, which is the bedrock for our thesis. We expect the company to submit some level of eGFR data during 2023 for accelerated approval; if that crosses FDA's threshold, FDA can approve the candidate just based on the 9-month data from ALIGN.
We are bullish on phase 3 ALIGN data and we believe Atrasentan will likely be a bigger player in IgAN over TVTX's Sparsentan
We note that the phase 3 ALIGN study enrolled IgAN patients who are on maximally tolerated, optimized RASi therapy (unless the patient is RASi intolerant) and used a placebo arm (even though we expect most of the patients to be on RASi therapy). We find this trial design superior to the Travere Therapeutics, Inc. (TVTX) PROTECT trial which specified ACEi as a control arm (and protocolized it), which increases the bar for Sparsentan to succeed. This may explain why the placebo proteinuria was extremely high for the SPAR trials, as some patients who entered the trial may have increased their Irbesartan dose further as their dose that they thought was the "max tolerated dose" is in fact not the max tolerated dose meeting the protocolized definition during TVTX's trial.
In addition, in Atrasentan's ALIGN trial, patients who are intolerant may be enrolled on the placebo arm, but for TVTX's trial that may not be possible; Atrasentan has an easier bar than SPAR. In principle, the Atrasentan trial will be easier to show placebo/control adjusted proteinuria and eGFR. Furthermore, Sparsentan uses a weaker ERA over Sparsentan and used lower doses vs. FSGS trial, which further complicates the picture as the chance of Sparsentan showing "robust enough" eGFR can be trickier, even though robust proteinuria can be achieved. Furthermore, Atrasentan comes with an additional convenience advantage as it can be mixed and matched with generic RASi (ACEi and ARBs) and prescribers can adjust the dosing (especially for patients with a high risk of hypotension or low eGFR under 30), which adds to the convenience compared to Sparsentan which has one set dose.
Things get messy, especially when patients with low eGFR or hyperkalemia as RASi tend to aggravate the complication related to it. Furthermore, combination drugs will have additional complexity when patients start or get off SGLT-2's which also reduces blood pressure. We think this will make reimbursement and pricing more complex for Sparsentan even with the approval.
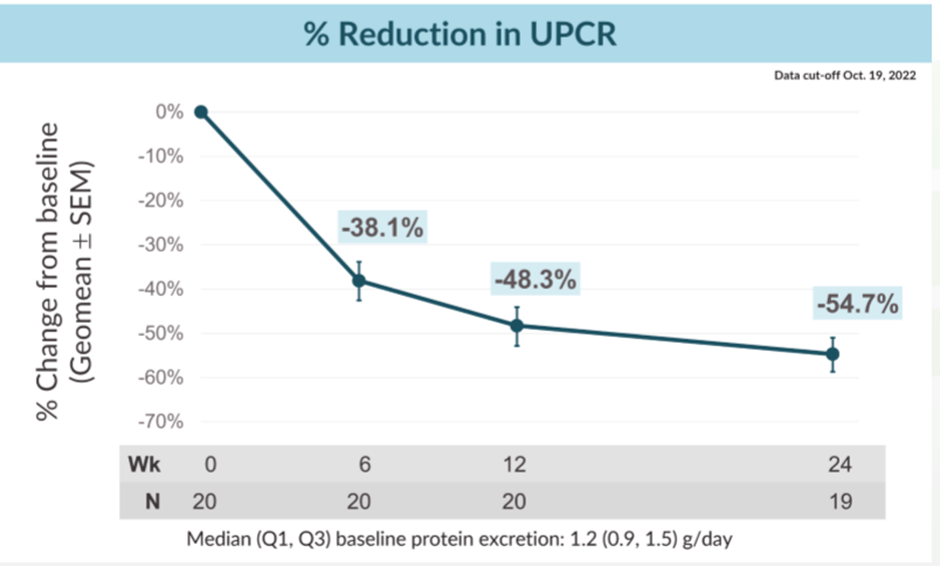
Phase 2 AFFINITY trial showed robust ~54.7% proteinuria reduction at week 24
The AFFINITY Study (see www.clinicaltrials.gov, identifier NCT04573920) is an ongoing global phase 2, open-label, basket study to evaluate the efficacy and safety of Atrasentan in patients with the proteinuric glomerular disease who are at risk of progressive loss of renal function. The four AFFINITY cohorts consist of patients with biopsy-proven IgAN with urine protein to creatinine ratio ((UPCR)) of 0.5 to 1.0 g/g, focal segmental glomerulosclerosis ((FSGS)), Alport syndrome, and diabetic kidney disease ((DKD)) in combination with an SGLT2 inhibitor. The 20 patients enrolled in each cohort receive 0.75 mg oral atrasentan daily for 52 weeks while continuing to receive a maximally tolerated and stable dose of a RAS inhibitor as the standard of care. Source: Company .
We note that Atrasentan showed almost best-in-class proteinuria reduction (around 54.7% at week 24), although the trial had a small sample size of 20 patients. Using a historical placebo proteinuria reduction of 5-15%, we get almost 40-50% proteinuria reduction, which is highly impressive and definitely above the threshold for accelerated approval. We think the bar for most studies is budgeted to show a 30% reduction by looking at how trials are powered and based on TARPEYO's accelerated approval with around 27% proteinuria reduction (placebo adjusted) at month 9.
We believe this bodes well for the drug moving forward in the ALIGN trial. Last Nov , KDNY released additional data from its AFFINITY trial; interestingly, the trial did not show any eGFR benefits and noted "suggesting proteinuria reductions were not primarily due to hemodynamic effects of atrasentan." This makes us believe that ERA's additional mechanism of action (on top of RASi) may not lead to additional eGFR benefits (additional proteinuria benefit can be driven by ERA's direct action on the kidney, such as increasing absorption of albumin) or that 24 weeks was too short of showing material enough eGFR improvement or the trial size was too small. Either way, including patients who are intolerant to RASi and not protocolizing the supportive care arm with maximum tolerable RASi dose should make it easier to show superior proteinuria and eGFR benefits during the phase 3 ALIGN trial compared to Travere's ( TVTX ) phase 3 PROTECT (upcoming PDUFA in Q1 2023).
TVTX's PROTECT trial is the only IgAN trial that protocolized the maximization of irbesartan, and we think this protocolization is a very important differentiation, as without protocolizing, many patients may enroll in a study without "truly maximum RASi." What individual physician would deem as maximum tolerable dose may not be actually the max dose that the patient can tolerate, which may explain why placebo proteinuria reduction was so high in Sparsentan trials even though all patients enrolled should start the treatment with "stable maximal tolerable dose."
{kind=link}
Atrasentan's safety seems robust
Based on the APRIL 2022 cutoff, Atrasentan looks like it is well-tolerated, with no treatment-related serious side effects and minimal edema, which is a class-wide side effect. On a positive note, we believe that with the increase in usage of SGLT-2 across the board, edema will be less of a concern as SGLT-2 can reduce edema. Also, we note that Atrasentan lacks the Sulfonamide group, unlike Travere's Sparsentan; as such, it may be able to avoid potential REMS monitoring requirements or black-boxed warnings that Sparsentan is facing. However, we concede that due to the limited sample size (n=20) and short trial duration, we need larger and longer-term data to build a high degree of conviction around the class's safety. However, having a straightforward and tried and tested ERA (used in PAH as a standard of care) is more comforting than a novel ERA+ACEi combination in one pill.
- One patient discontinued study treatment due to a headache, which was considered a moderate related adverse event by the investigator, and one patient completed 52 weeks of treatment.
- One patient had an unrelated serious adverse event of a traffic accident.
- Five patients had a treatment-related adverse event, all of which were considered mild or moderate.
- Two patients experienced peripheral edema - one mild and one moderate - which resolved in less than seven days with the temporary use of low-dose diuretics.
- All other treatment-emergent adverse events have resolved. Source: Company publication .
BION-1301 exciting anti-APRIL therapy
BION-1301's proteinuria reduction of ~53% within 24 weeks was robust. Limitation in sample size (n=8) notwithstanding, we find the data highly positive, especially considering the fact that they are enrolling more patients in the SC study. We believe subcutaneous ((SC)) dosage forms offer significantly superior convenience than the IV dosage form, and so far the proteinuria reduction between SC and IV arms looks comparable. Also, we point at consistency in the anti-APRIL pathway, BION-1301, VIS649, Sibeprenlimab from Otsuka, and Telitacicept from Remegen all showed consistent proteinuria reduction and the data is almost superimposable in terms of immunoglobulin reduction, proteinuria, and eGFR, although, Vera Therapeutics, Inc.'s ( VERA ) JANUS study had some noise around the 75mg arm (likely driven by couple outliers). We find this consistency in biomarker data and clinical outcomes highly promising. Also, the jury is out regarding anti-APRIL and anti-APRIL/Blys (dual pathway), especially with Vera's lackluster proteinuria reduction of ~30% at week 36 even with the high dose (150mg). This makes us think that additional benefits coming from Blys that prevent B cells from maturing and producing immunoglobulin may not provide immediate benefit in the short term or it could just be an Atacicept-specific MOA issue. Furthermore, if proteinuria and eGFR stabilization are comparable or slightly inferior, we would prefer anti-APRIL monotherapy as it will likely have a better safety profile, especially around infection, as the anti-APRIL/Blys pathway has shown higher infection rates in previous trials (especially lower respiratory infections, cases of pneumonia, etc.). This potential infection risk may mean that FDA or EMA may require "vaccination requirements" like the complement inhibitors, which can further hamper the market adoption as it adds additional hurdles for prescribers.
BION-1301 trial design ( Company)
Valuation: Best risk-reward in the IgAN space
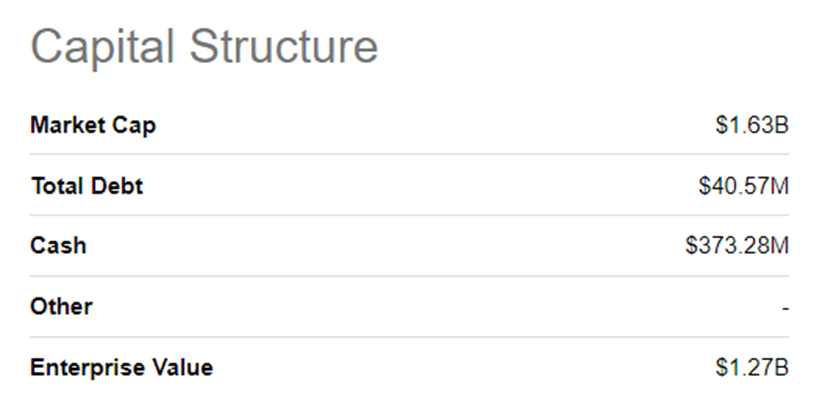
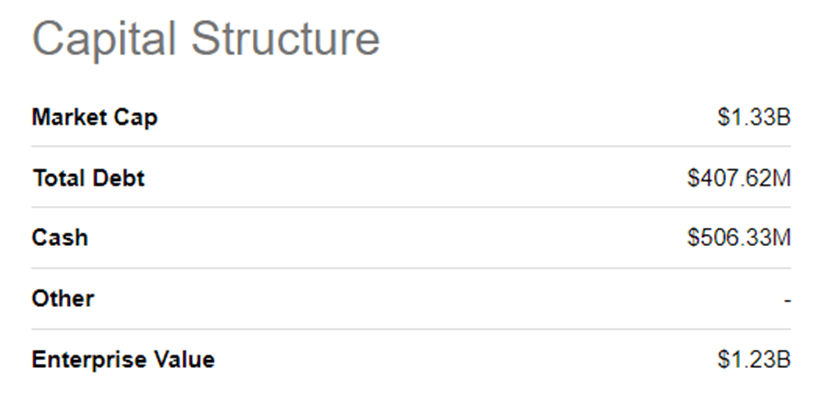
We like KDNY more than TVTX as KDNY has two robust candidates, BION-1301 and Atrasentan, and the two companies have similar enterprise value. Even though TVTX's Sparsentan will be 1-2 years earlier to the market (if it gets approved, although we are neutral to bearish on TVTX's approval), we still think Atrasentan to be able to reach comparable or higher peak sales due to its convenience advantages. Even in the worst case, even if Atrasentan's phase 3 ALIGN fails, we believe KDNY has additional pipeline value from BION-101 to fall back on, compared to TVTX that only has Sparsentan and is almost positioned as a binary IgAN play, especially with the FDA dinging them for "not showing enough eGFR benefit" in their phase 3 FSGS trial.
SA KDNY valuation (Seeking Alpha) SA TVTX valuation (Seeking Alpha)
{kind=link}
{kind=link}
Risks
Regulatory, clinical risk, commercial risk, and cash runway risk, considering KDNY is a pre-commercial biotech and a first-time launcher. However, we believe KDNY can benefit from TVTX (both positive and negative) or VERA's readout.
Conclusion
We are long Chinook Therapeutics, Inc. due to a good risk-reward set-up and modest valuation for a company with best-in-class ERA and anti-APRIL pipeline. We like the standalone ERA and anti-APRIL as a mechanism of action due to the higher degree of convenience and a lesser degree of safety overhang. Furthermore, we expect positive readthroughs from upcoming readouts from TVTX (Feb 2023) and VERA (which were negative).
For further details see:
Chinook Therapeutics: Best Biotech For Kidney Disease Exposure, With Catalysts